Department of Neurosurgery, Ewha Womans University School of Medicine, Seoul, Korea.
Corresponding author: Myung-Hyun Kim, Department of Neurosurgery, Ewha Womans University School of Medicine, 1071 Anyangcheon-ro, Yangcheon-gu, Seoul 158-710, Korea. Tel: 82-2-2650-5088, Fax: 82-2-2650-5088, kimmh@ewha.ac.kr
• Received: July 31, 2012 • Accepted: October 15, 2012
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Anterior microforaminotomy (AMF) is an alternative procedure to treat unilateral cervical pathology. Although the results have been reported favorable in the previous studies, postoperative degeneration may occur. We analyze long-term outcome to determine the critical size of AMF.
Methods
A retrospective study was performed. Clinical data with chart review, radiologic data with picture archiving and communication system (PACS) images were obtained. Long-term clinical outcomes were accessed by a questionnaire, including visual analogue scale (VAS) and neck disability index (NDI). Various clinical, radiological data were statistically analyzed.
Results
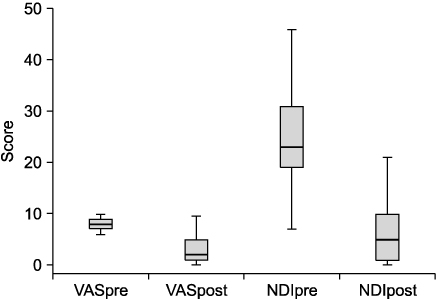
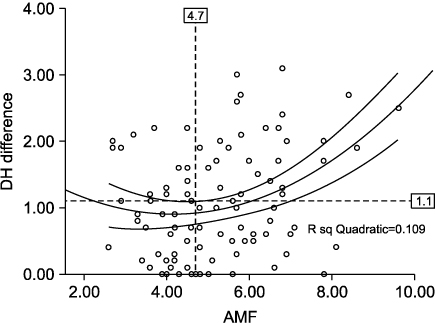
Eight-two patients were enrolled in this study. Main pathology was spondylotic spur (53.7%), soft disc herniation (36%). Mean age was 49 years old. There was no surgery-related complication. Mean follow-up was 6.1 years. 90.3% showed favorable clinical outcome. Mean VAS score was decreased from 8.2 to 2.9, and NDI score was decreased from 24.5 to 6.7 (P<0.05). 88.7% showed decrease of disc height (DH), and mean change was 1 mm. DH change was correlated positively with the disc invasion and AMF diameter (P<0.05). Mean diameter of AMF was 5.2 mm. According to statistical analysis, the critical diameter of AMF was 4.7 mm, directly affecting DH decrease. Any radiological parameters did not affect the clinical outcome.
Conclusion
AMF was an effective procedure to treat unilateral cervical pathology. Critical DH decreases and/or disc invasion may be the trigger of sequential degeneration. To preserve DH, AMF diameter should be small and disc invasion should be avoided.
1. Bertalanffy H, Eggert HR. Clinical long-term results of anterior discectomy without fusion for treatment of cervical radiculopathy and myelopathy: a follow-up of 164 cases. Acta Neurochir (Wien) 1988;90:127-135.
4. Mosdal C. Cervical osteochondrosis and disc herniation. Eighteen years' use of interbody fusion by Cloward's technique in 755 cases. Acta Neurochir (Wien) 1984;70:207-225.
7. Baba H, Furusawa N, Imura S, Kawahara N, Tsuchiya H, Tomita K. Late radiographic findings after anterior cervical fusion for spondylotic myeloradiculopathy. Spine 1993;18:2167-2173.
8. Elsawaf A, Mastronardi L, Roperto R, Bozzao A, Caroli M, Ferrante L. Effect of cervical dynamics on adjacent segment degeneration after anterior cervical fusion with cages. Neurosurg Rev 2009;32:215-224.
9. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528.
10. Hussain M, Natarajan RN, An HS, Andersson GB. Motion changes in adjacent segments due to moderate and severe degeneration in C5-C6 disc: a poroelastic C3-T1 finite element model study. Spine 2010;35:939-947.
11. Nassr A, Lee JY, Bashir RS, Rihn JA, Eck JC, Kang JD, et al. Does incorrect level needle localization during anterior cervical discectomy and fusion lead to accelerated disc degeneration? Spine 2009;34:189-192.
13. Schwab JS, Diangelo DJ, Foley KT. Motion compensation associated with single-level cervical fusion: where does the lost motion go? Spine 2006;31:2439-2448.
16. Snyder GM, Bernhardt M. Anterior cervical fractional interspace decompression for treatment of cervical radiculopathy: a review of the first 66 cases. Clin Orthop Relat Res 1989;246:92-99.
17. Jho HD. Microsurgical anterior cervical foraminotomy for radiculopathy: a new approach to cervical disc herniation. J Neurosurg 1996;84:155-160.
19. Choi G, Lee SH, Bhanot A, Chae YS, Jung B, Lee S. Modified transcorporeal anterior cervical microforaminotomy for cervical radiculopathy: a technical note and early results. Eur Spine J 2007;16:1387-1393.
20. Cornelius JF, Bruneau M, George B. Microsurgical cervical nerve root decompression via an anterolateral approach: clinical outcome of patients treated for spondylotic radiculopathy. Neurosurgery 2007;61:972-980.
21. Hong WJ, Kim WK, Park CW, Lee SG, Yoo CJ, Kim YB, et al. Comparison between transuncal approach and upper vertebral transcorporeal approach for unilateral cervical radiculopathy - a preliminary report. Minim Invasive Neurosurg 2006;49:296-301.
22. Jho HD, Kim WK, Kim MH. Anterior microforaminotomy for treatment of cervical radiculopathy: part 1--disc-preserving "functional cervical disc surgery". Neurosurgery 2002;51:5 Suppl. S46-S53.
25. Lee JY, Lohr M, Impekoven P, Koebke J, Ernestus RI, Ebel H, et al. Small keyhole transuncal foraminotomy for unilateral cervical radiculopathy. Acta Neurochir (Wien) 2006;148:951-958.
26. Saringer W, Nöbauer I, Reddy M, Tschabitscher M, Horaczek A. Microsurgical anterior cervical foraminotomy (uncoforaminotomy) for unilateral radiculopathy: clinical results of a new technique. Acta Neurochir (Wien) 2002;144:685-694.
30. Kotani Y, McNulty PS, Abumi K, Cunningham BW, Kaneda K, McAfee PC. The role of anteromedial foraminotomy and the uncovertebral joints in the stability of the cervical spine. A biomechanical study. Spine 1998;23:1559-1565.
32. Okada E, Matsumoto M, Ichihara D, Chiba K, Toyama Y, Fujiwara H, et al. Aging of the cervical spine in healthy volunteers: a 10-year longitudinal magnetic resonance imaging study. Spine 2009;34:706-712.
34. Osti OL, Vernon-Roberts B, Fraser RD. Anulus tears and intervertebral disc degeneration: an experimental study using an animal model. Spine 1990;15:762-767.
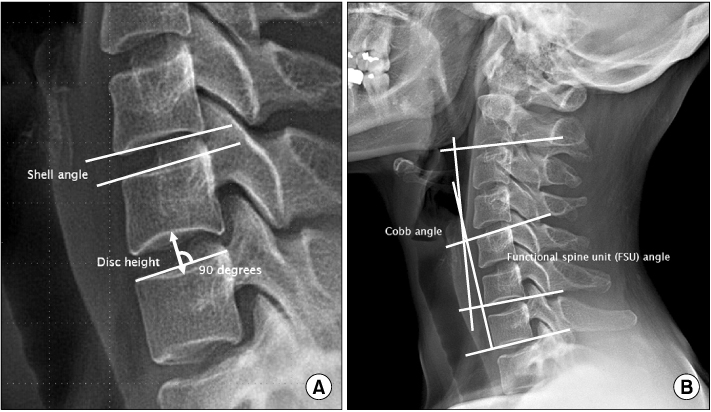
(A) Measurement of disc height (DH) and shell angle (SA) on a plain radiograph in neutral lateral position. (B) Functional spine unit (FSU) and Cobb angles.
Fig. 2
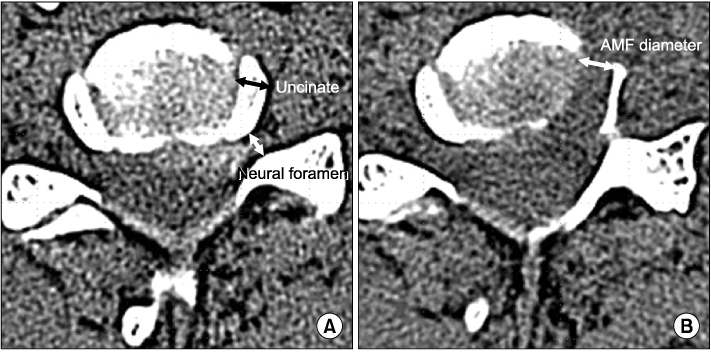
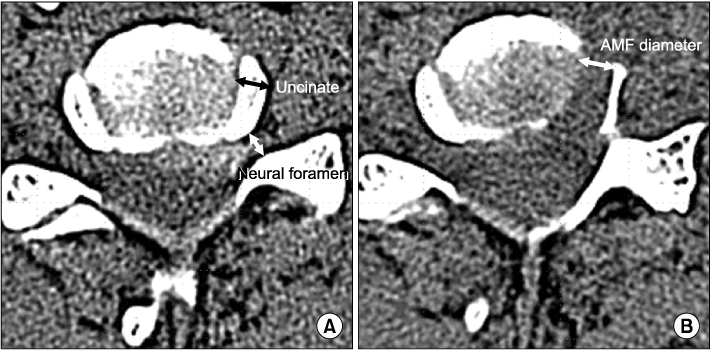
(A) Diameter of the uncinate process is measured at the preoperative axial CT image showing the widest area of the disc. Diameter of the neural foramen was measured at the point just medial to the fossa locating the dorsal root ganglion. (B) Diameter of anterior microforaminotomy is measured on the postoperative axial CT image. AMF, anterior microforaminotomy.
Fig. 3
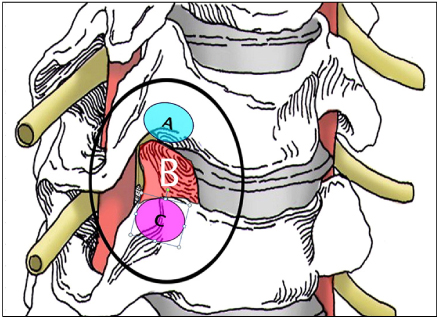
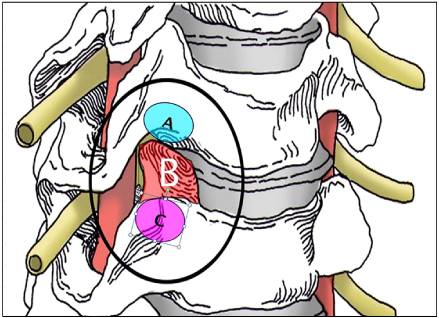
Illustration showing the various entry and resection sites of microforaminotomy. (A) Entry point of upper transcorporeal approach. (B) Resection site of transuncal approach. (C) Entry point of lower transcorporeal approach.
Fig. 4
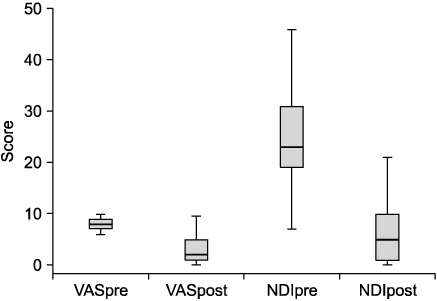
Box-plot graph showing preoperative and postoperative changes of visual analog scale (VAS) and neck disability index (NDI) scores with mean, maximum, and minimum values. VASpre, preoperative VAS; VASpost, postoperative VAS; NDIpre, preoperative NDI; NDIpost, postoperative NDI.
Fig. 5
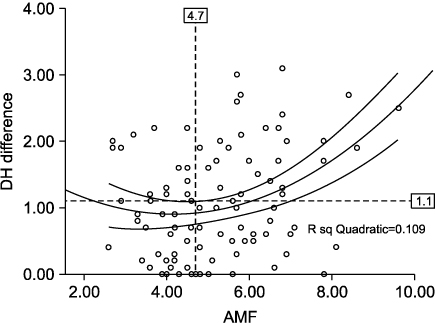
Graph showing correlation between the anterior microforaminotomy (AMF) diameter and changes in postoperative disc height (DH). Curvilinear lines indicate the trend line with 95% confidence lines extracted by quadratic regression analysis. The critical AMF diameter is 4.7 mm, above which the DH difference will increase remarkably as the AMF diameter increases.
Fig. 6
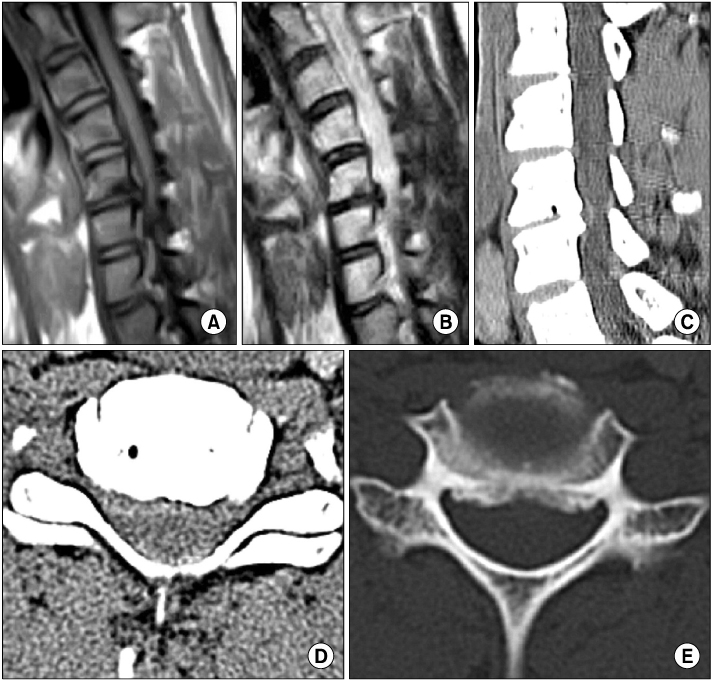
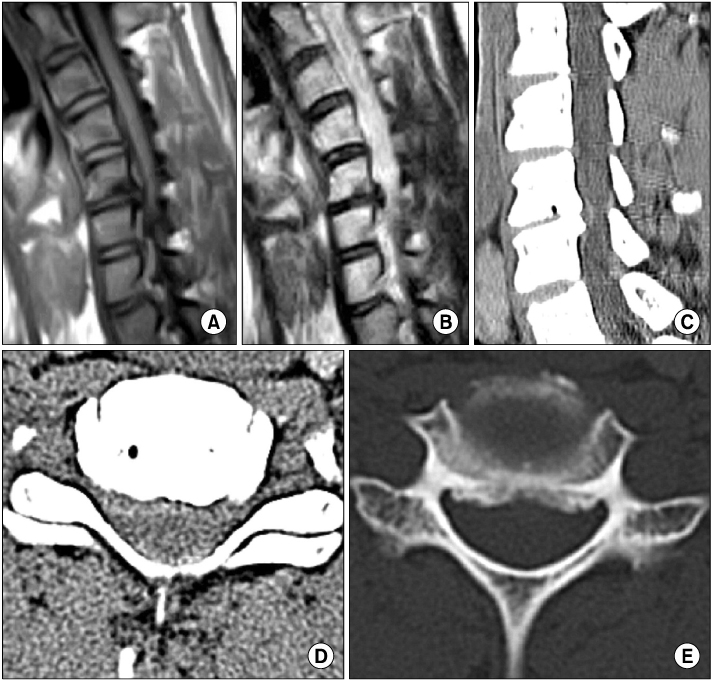
Preoperative CT and sagittal MR images. (A~C) Sagittal T1 and T2 MRI and CT images showing disc protrusion with spur at the C5-6 level. (D, E) Axial CT images showing combined disc and spur compression at the right neural foramen.
Fig. 7
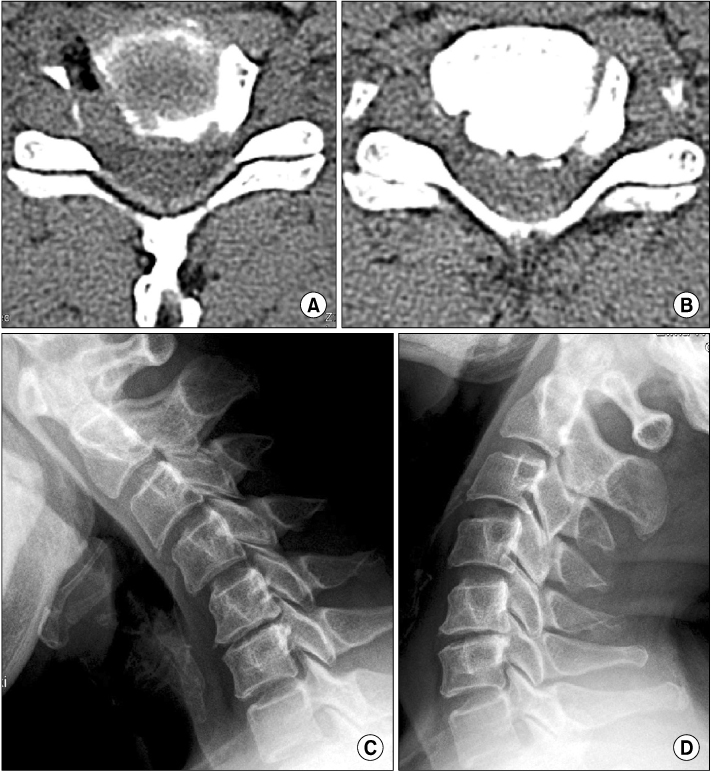
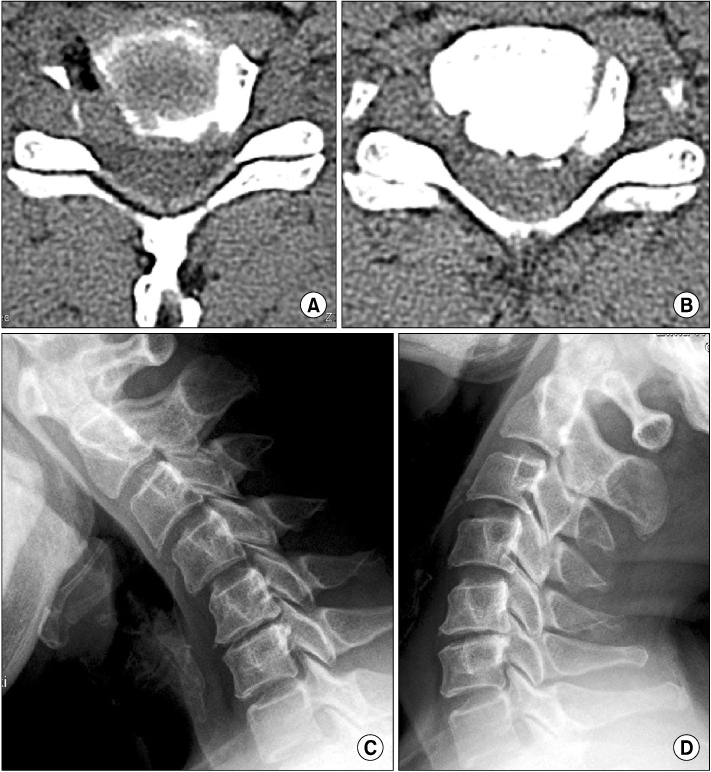
Postoperative axial CT images and dynamic plain radiographs. (A) Immediate postoperative axial CT image showing foraminotomy on the right side. (B) Axial CT image showing new bone formation around the margin of the foraminotomy at a follow-up of 5 years. (C, D) Plain extension and flexion X-rays showing well-preserved cervical motion.
Table 1
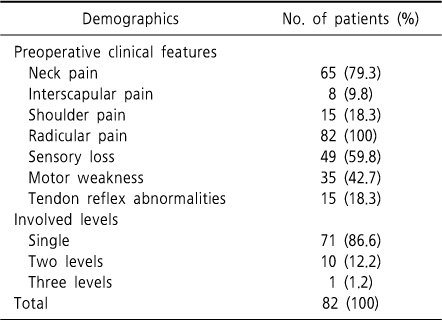
Preoperative clinical features and levels of lesion
Does the Size of Anterior Microforaminotomy Affect the Surgical Outcome?
Fig. 1
(A) Measurement of disc height (DH) and shell angle (SA) on a plain radiograph in neutral lateral position. (B) Functional spine unit (FSU) and Cobb angles.
Fig. 2
(A) Diameter of the uncinate process is measured at the preoperative axial CT image showing the widest area of the disc. Diameter of the neural foramen was measured at the point just medial to the fossa locating the dorsal root ganglion. (B) Diameter of anterior microforaminotomy is measured on the postoperative axial CT image. AMF, anterior microforaminotomy.
Fig. 3
Illustration showing the various entry and resection sites of microforaminotomy. (A) Entry point of upper transcorporeal approach. (B) Resection site of transuncal approach. (C) Entry point of lower transcorporeal approach.
Fig. 4
Box-plot graph showing preoperative and postoperative changes of visual analog scale (VAS) and neck disability index (NDI) scores with mean, maximum, and minimum values. VASpre, preoperative VAS; VASpost, postoperative VAS; NDIpre, preoperative NDI; NDIpost, postoperative NDI.
Fig. 5
Graph showing correlation between the anterior microforaminotomy (AMF) diameter and changes in postoperative disc height (DH). Curvilinear lines indicate the trend line with 95% confidence lines extracted by quadratic regression analysis. The critical AMF diameter is 4.7 mm, above which the DH difference will increase remarkably as the AMF diameter increases.
Fig. 6
Preoperative CT and sagittal MR images. (A~C) Sagittal T1 and T2 MRI and CT images showing disc protrusion with spur at the C5-6 level. (D, E) Axial CT images showing combined disc and spur compression at the right neural foramen.
Fig. 7
Postoperative axial CT images and dynamic plain radiographs. (A) Immediate postoperative axial CT image showing foraminotomy on the right side. (B) Axial CT image showing new bone formation around the margin of the foraminotomy at a follow-up of 5 years. (C, D) Plain extension and flexion X-rays showing well-preserved cervical motion.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Does the Size of Anterior Microforaminotomy Affect the Surgical Outcome?
Preoperative clinical features and levels of lesion
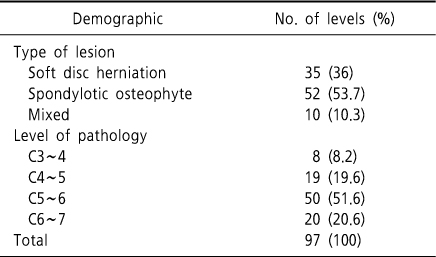
Type of lesion and level of pathology
Table 1
Preoperative clinical features and levels of lesion