Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea.
1Department of Pathology, The Catholic University of Korea College of Medicine, Seoul, Korea.
Copyright © 2014. Ewha Womans University School of Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
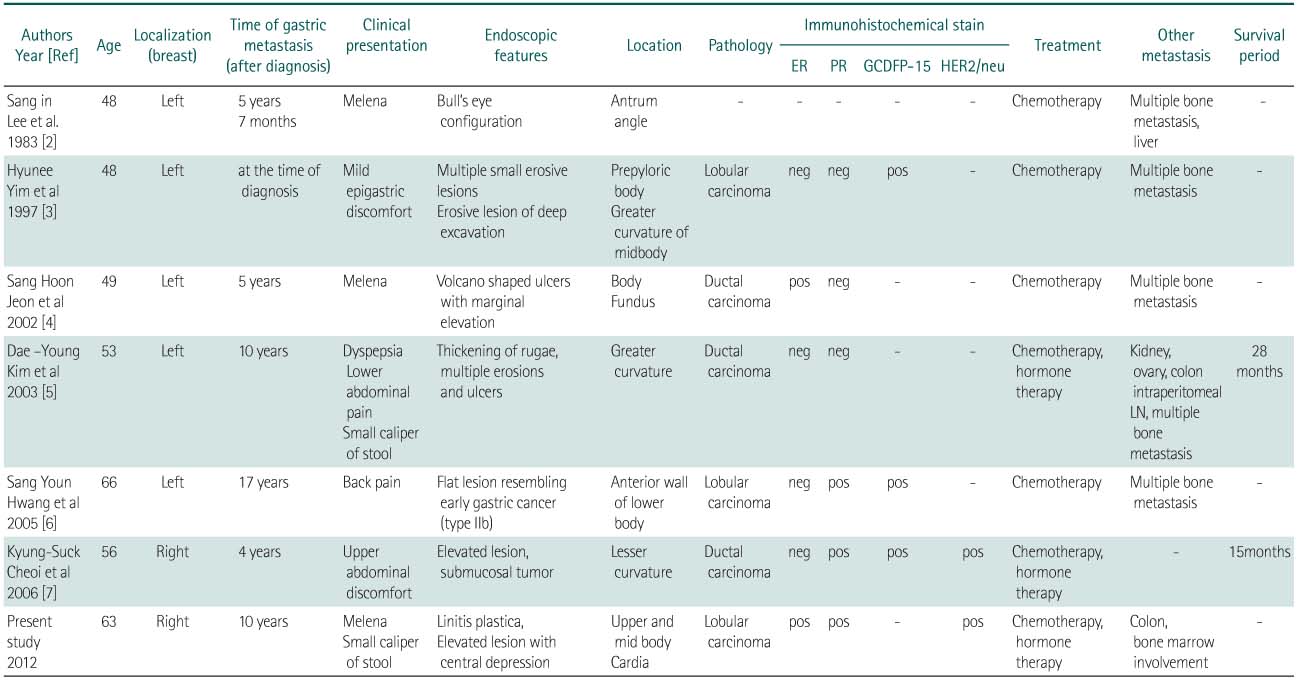
Clinical characteristics of 7 patients with gastric metastasis of breast cancer in Korea
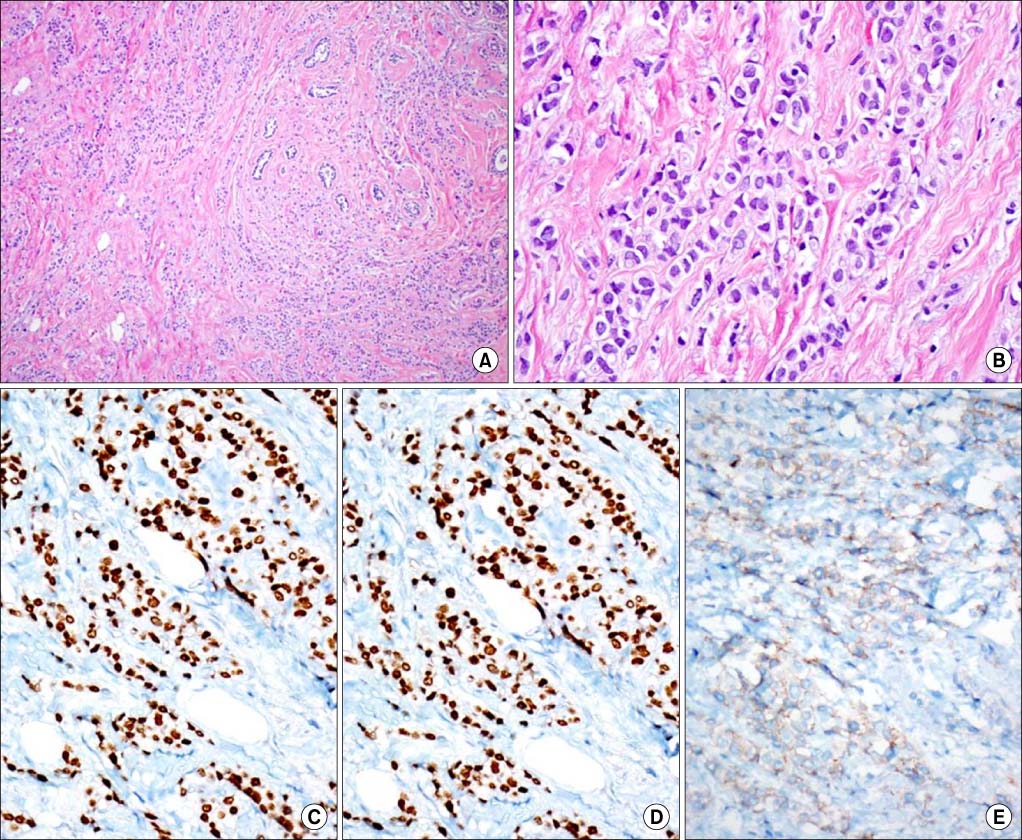
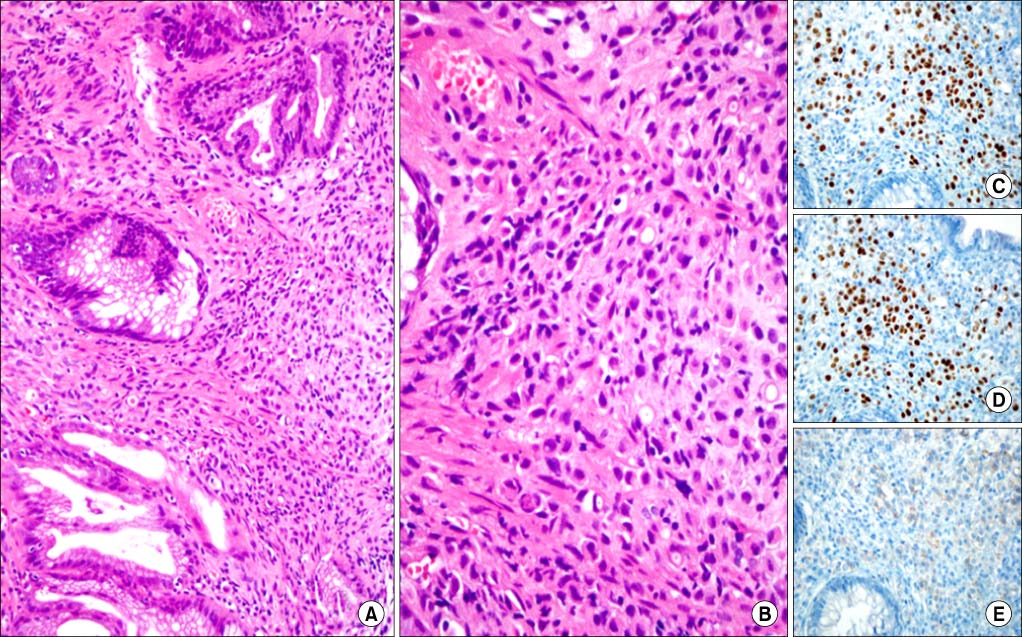
ER, estrogen receptor; PR, progesterone receptor; GCDFP-15, gross cystic disease fluid protein 15.
ER, estrogen receptor; PR, progesterone receptor; GCDFP-15, gross cystic disease fluid protein 15.