1Department of Occupational and Environmental Medicine, Inha University College of Medicine, Incheon, Korea
2Korea Occupational Diseases Surveillance Center, Inha University Hospital, Incheon, Korea
3Department of Occupational and Environmental Medicine, Hanyang University College of Medicine, Seoul, Korea
4Korea Occupational Diseases Surveillance Center, Hanyang University Hospital, Seoul, Korea
5Graduate School of Public Health, Hanyang University, Seoul, Korea
6Department of Occupational and Environmental Medicine, Chungbuk National University College of Medicine, Cheongju, Korea
7Korea Occupational Diseases Surveillance Center, Chungbuk National University Hospital, Cheongju, Korea
8Korea Occupational Diseases Surveillance Center, Hanyang University Guri Hospital, Guri, Korea
9Department of Occupational and Environmental Medicine, Keimyung University School of Medicine, Daegu, Korea
10Korea Occupational Diseases Surveillance Center, Keimyung University Dongsan Medical Center, Daegu, Korea
11Department of Occupational and Environmental Medicine, Ajou University School of Medicine, Suwon, Korea
12Korea Occupational Diseases Surveillance Center, Ajou University Hospital, Suwon, Korea
13Department of Occupational and Environmental Medicine, Kosin University College of Medicine, Busan, Korea
14Korea Occupational Diseases Surveillance Center, Kosin University Gospel Hospital, Busan, Korea
15Department of Occupational and Environmental Medicine, Wonju College of Medicine, Wonju Severance Christian Hospital, Yonsei University, Wonju, Korea
16Korea Occupational Diseases Surveillance Center, Wonju College of Medicine, Wonju, Korea
17Department of Preventive, and Occupational & Environmental Medicine, School of Medicine, Pusan National University, Yangsan, Korea
18Department of Occupational and Environmental Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea
19Korea Occupational Diseases Surveillance Center, Pusan National University Yangsan Hospital, Yangsan, Korea
20Department of Occupational and Environmental Medicine, Hanyang University Guri Hospital, Guri, Korea
21Department of Occupational and Environmental Medicine, Kosin University Gospel Hospital, Busan, Korea
22Department of Occupational and Environmental Medicine, Keimyung University School of Medicine, Daegu, Korea
23Department of Occupational and Environmental Medicine, Hanyang University Hospital, Korea
24Department of Occupational and Environmental Medicine, Chosun University School of Medicine, Gwangju, Korea
25Korea Occupational Diseases Surveillance Center, Chosun University Hospital, Gwangju, Korea
*Corresponding author: Inah Kim,
Department of Occupational and Environmental Medicine, Hanyang University
College of Medicine, 222 Wangsimni-ro, Seongdong-gu, Seoul 04763, Korea, E-mail:
inahkim@hanyang.ac.kr
• Received: December 2, 2024 • Revised: January 9, 2025 • Accepted: January 9, 2025
This is an Open-Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits
unrestricted non-commercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
This review examines the challenges associated with occupational disease
surveillance in Korea, particularly emphasizing the limitations of current data
sources such as the Industrial Accident Compensation Insurance (IACI) statistics
and special health examinations. The IACI system undercounts cases due to its
emphasis on severe diseases and restrictions on approvals. Special health
examinations, although they cover a broad workforce, are constrained by their
annual scheduling, which leads to missed acute illnesses and subclinical
conditions. The paper also explores the history of occupational disease
surveillance in Korea, highlighting the fragmented and disease-specific approach
of earlier systems. The authors introduce the newly established Korea
Occupational Disease Surveillance Center (KODSC), a comprehensive nationwide
system designed to gather, analyze, and interpret data on occupational diseases
through a network of regional centers. By incorporating hospital-based
surveillance and focusing on acute poisonings and other sentinel events, the
KODSC aims to overcome the limitations of previous systems and promote
collaboration with various agencies. Although it is still in the early stages of
implementation, the KODSC demonstrates potential for improving data accuracy and
contributing valuable insights for public health policy.
Korea began its industrialization in the 1960s, leading to the construction of
numerous factories throughout the 1970s and 1980s. As a result, coal mining
expanded significantly to meet the energy demands of the manufacturing industry
and to provide a source of home heating. The manufacturing processes involved
the use of various chemicals. This shift towards a manufacturing-based economy
has been associated with several occupational diseases, including carbon
disulfide and heavy metal poisoning [1].
In recent years, Korea has achieved global competitiveness in several sectors,
including mobile phones, semiconductors, automobiles, chemicals, and steel
manufacturing. Additionally, Korean cultural content such as music, gaming, and
webtoons has become a vital industry, playing a pivotal role in the national
economy. Despite these advancements, the manufacturing sector remains the
largest in terms of gross domestic product (GDP), followed by sales and retail
[2].
Despite Korea's impressive economic growth, occupational injuries continue
to pose a significant problem. By 2022, the rate of fatal occupational injuries
per 100,000 workers is projected to be 4.33. This figure is substantially higher
than Japan's rate of 1.54 and Germany's 0.84, placing Korea among
the higher ranks of International Labour Organisation (ILO) member countries
[3]. The ILO reports that
approximately 2.3 million women and men globally die each year from work-related
accidents or diseases, which equates to over 6,000 deaths daily. Furthermore,
around 340 million occupational accidents and 160 million cases of work-related
illnesses are recorded annually worldwide [4].
Recent Global Burden of Disease research has concentrated on the impact of
occupational factors; however, this impact is relatively minor in high-income
countries. Determining the burden of occupational diseases presents significant
challenges, particularly due to the incubation period of chronic diseases, high
turnover rates in flexible labor markets, and the necessity for reliable
information to confirm exposure [5].
Identifying cases linked to occupational factors is crucial for compiling these
data, which are vital for public health. Routine surveillance systems, such as
the Health and Occupation Research (THOR) network, play a key role in providing
important data sources [6].
Objectives
This review examines the importance of establishing a routine surveillance scheme
as a foundational framework for comprehending the burden of occupational
diseases. It also describes the occupational disease surveillance system that
was recently implemented in Korea.
Ethics statement
As this study is a literature review, it did not require institutional review board
approval or individual consent.
Occupational disease and surveillance
The term "surveillance" originates from a French word meaning
"to watch over" [7]. It is
defined as the continuous, systematic collection, analysis, and interpretation of
health-related data that are crucial for the planning, implementation, and
evaluation of public health practices. This process is tightly linked with the
prompt dissemination of these data to individuals responsible for prevention and
control measures [8]. The goal of surveillance
is to supply information that public health personnel, government leaders, and the
community can use to inform public health policies and programs [9,10].
It is important to utilize multiple data sources to accurately gauge the prevalence
of occupational diseases. In Korea, the Industrial Accident Compensation Insurance
(IACI) statistics serve as one such source for tracking the number of occupational
diseases. However, this system only allows claims for severe diseases, and
approximately two-thirds of these claims are approved. Consequently, the IACI
statistics may not fully represent the actual incidence of occupational diseases.
Additionally, the disparity between the ratios of fatal to non-fatal cases in
occupational injuries and illnesses indicates that some data might be missing [11].
In 2022, statistics approved by the IACI indicated that 23,134 individuals were
recognized as having occupational or work-related diseases. Although this figure
might initially appear substantial, a deeper analysis highlights several concerning
issues. More than half of these cases were attributed to musculoskeletal disorders,
deaths from cardio- or cerebrovascular diseases due to overwork, and mental
illnesses. Noise-induced hearing loss was responsible for 5,376 cases, while
pneumoconiosis accounted for 1,679 cases [12]. Given the presence of 600,000 manufacturing workplaces and 3.4 million
workers in Korea, the reported 553 cases related to exposure to hazardous chemicals
seem implausibly low. This significant discrepancy points to a potential shortfall
in the current system's ability to capture a comprehensive range of
occupational diseases.
Another source of occupational disease surveillance is special health examinations.
These are occupational health screening tests designed for the early detection of
selected occupational diseases in workers. It is mandatory for employees exposed to
181 risk factors, including hazardous chemicals, gases, physical risk factors, and
night work, to undergo these examinations. To date, almost 2.2 million workers have
been examined under this system. However, due to the nature of medical examinations,
which are typically conducted at one-year intervals based on exposure to specific
physical and chemical hazards, they are useful in identifying chronic diseases in
workers who have been employed for more than one year. Nonetheless, they have
limitations in identifying subclinical conditions or diseases that may manifest
acutely in the absence of a clinical examination [13]. Periodic health examinations cannot detect acute illnesses or
subclinical conditions and require workers to have been employed at a workplace for
more than a year. Consequently, short-term or day laborers who frequently change
workplaces are not included in the statistics. This system also overlooks
small-scale workplaces and foreign laborers. The most commonly observed conditions
(95%) are pneumoconiosis and noise-induced hearing loss, with examinations typically
conducted annually. This frequency makes it challenging to detect diseases that
arise acutely. Indeed, an analysis of the rate of special health examinations in
workplaces with five or more employees revealed that less than 5% of manufacturing
workplaces had fewer than five employees, 20% of workplaces had between 5 and 49
employees, and 85% had 50 or more employees [14]. As a result, similar poisonings and deaths, such as those caused by
methanol [15], mercury [16], fire extinguishing agent HCFC-123 [17], and dichloromethane [18], have continued to occur until recently.
There are inherent gaps in Korea's occupational disease surveillance system
when it relies solely on compensation data from the IACI and special health
examinations. The current statistics on occupational diseases are inadequate for
understanding the full extent of this issue in South Korea. To adequately represent
and include vulnerable groups, it is crucial to establish surveillance systems based
on reporting and registration.
History of occupational disease surveillance
Awareness of occupational health issues has led to the development of various disease
surveillance systems, which are centered around specific diseases, regions, and
exposures. While these systems have achieved some of their intended outcomes during
their operational periods, the need for a more integrated approach has become
increasingly apparent. Among the most notable disease-focused surveillance systems
are those targeting asthma and lung cancer. A comprehensive overview of the
different surveillance systems implemented in Korea is detailed in Table 1. The Occupational Asthma Surveillance
System, the longest-running system of its kind in Korea, has been instrumental in
estimating the incidence of occupational asthma and identifying its major risk
factors [19]. Similarly, the lung cancer
surveillance system has been crucial in providing data on lung cancer cases,
highlighting the potential for prevention through reduced exposure to hazards in the
workplace [20].
Table 1.
History of the occupational disease surveillance system in Korea
Category
Details
Period
Occupational disease
surveillance
Disease-oriented
Asthma
1998−2002, 2004−2011
Musculoskeletal disorders
2000−2004
Skin disorders
1998
Mesothelioma and leukemia
2001
Mesothelioma
2002−2013
Lung cancer
2006−2010
Lymphohematopoietic disorders
2007−2010
Injury
2008−2011
Cerebro- and cardiovascular diseases
2010−2011
Region-oriented
Incheon
2001−2010
Busan, Ulsan, and Gyungnam
2001−2003, 2005−2010
Gumi
2002−2003
Changwon
2004
Jungbu-Nambu Regional Lung Cancer and
Leukemia
2011−2016
Exposure monitoring
Construction workers
2002
Needle stick injury
2009−2013
DMF (dimethylformamide) biological
exposure indices monitoring
Despite some achievements, funding for these surveillance systems was provided in a
fragmented manner, primarily through research grants, which posed challenges in
establishing a system capable of continuous operation. Furthermore, as researchers
developed disease-specific, hazard-specific, and regional surveillance systems,
inconsistencies arose in their definitions, scopes, and priorities. Consequently,
there is a growing need for a continuous, full-time, nationwide surveillance system.
With advancements in big data science and technology, there is an increasing
interest in developing a surveillance system that leverages regularly produced data,
adhering to legal regulations concerning occupational health. Efforts are underway
to create a carcinogen surveillance system utilizing national data, as well as a
system that integrates various national datasets [21–23].
However, the aforementioned limitations inherent in the national data suggest that
data-driven surveillance is not suitable for addressing urgent issues. Identifying
sentinel health events is crucial for the prevention and treatment of occupational
diseases [24]. This process also marks the
initial step in recognizing emerging occupational diseases or health hazards, such
as acute poisoning from newly developed industrial chemicals or unforeseen
exposures. The acute poisoning event discussed earlier exemplifies this issue.
Consequently, discussions are underway to establish a surveillance system
specifically tailored to acute poisoning. This system aims to prevent and identify
incidents caused by newly introduced industrial chemicals, beyond the previously
mentioned cases of methanol poisoning, dichloromethane poisoning, or HCFC-123.
The Occupational Acute Poisoning Disease Regional Surveillance Pilot Project, which
ran from 2016 to 2020, achieved significant outcomes, including the identification
of a case of toxic encephalopathy caused by 1,2-dichloropropane. This pilot project
utilized a mixed surveillance system that focused on region-specific diseases. The
results underscored the importance of implementing a hospital-based surveillance
system that involves direct interaction with patients to effectively detect acute
poisoning and occupational diseases. In response to these findings, the government
has decided to manage the surveillance system as a government-led initiative,
transitioning away from the previous research-oriented approach. However, due to the
challenges government agencies face in direct management, the system now operates
through partnerships with the Department of Occupational and Environmental Medicine
(OEM) and other clinical departments in major general hospitals, where patients
receive care.
New scheme for occupational disease surveillance
The Korea Occupational Disease Surveillance Center (KODSC) is a surveillance system
designed to collect, analyze, and interpret cases of occupational disease. It was
established in 2022, and by 2024, 10 regional centers were operational, in
accordance with the regional Ministry of Employment and Labor (MOEL) offices.
The missions of KODSC are as follows:
- Collect suspected cases of occupational disease reported by clinicians
- Carry out data production and management
- Perform workplace inspections and walk-through surveys to detect
occupational risk
- Provide medical consultations for occupational disease or injury cases of
MOEL regional offices
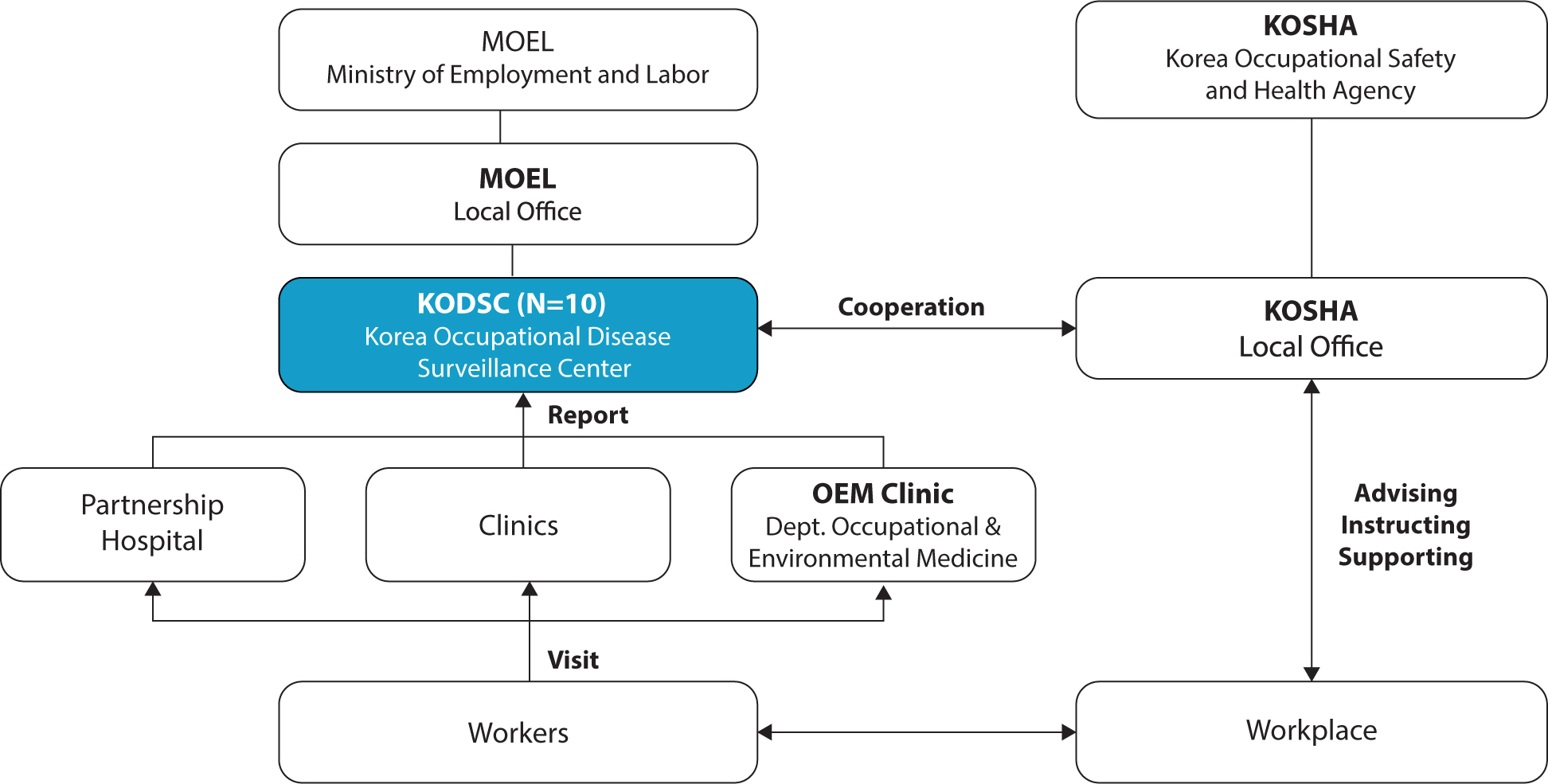
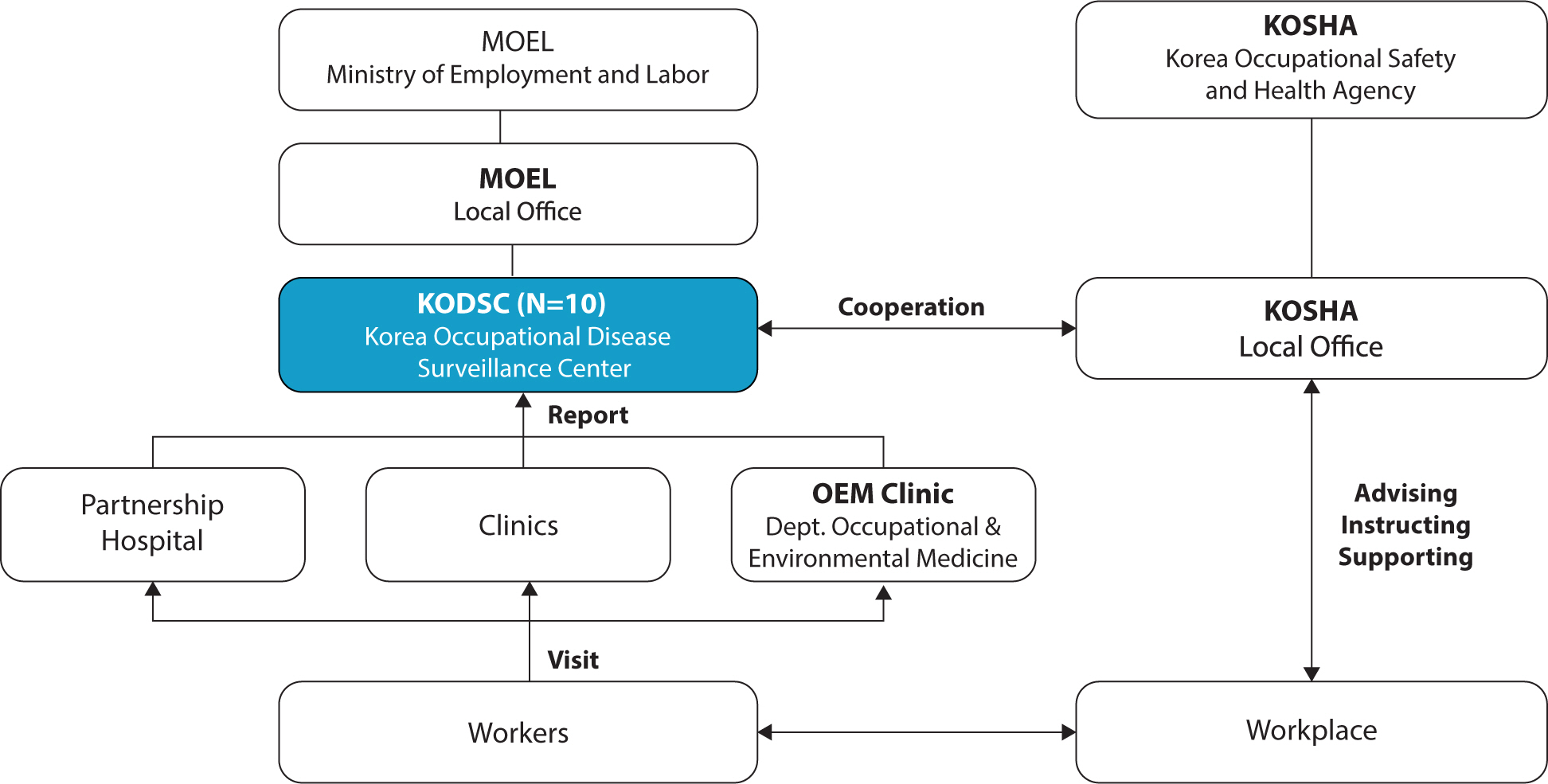
Fig. 1 shows the overall organizational chart. A
substantial component of this surveillance system is dedicated to gathering reports
of occupational diseases, including acute poisoning, from key emergency medical
facilities in the region. Although certain aspects of the current system may not be
monitored, it is expected that individuals will seek medical care at a hospital when
they feel unwell. The KODSC surveillance network system has been established across
ten regional centers. These centers are typically university hospitals, which are
the primary hospitals in their respective regions. They feature collaborations
between the Department of OEM and the Regional Emergency Medical Center, serving
both severe trauma patients and those with various other diseases.
Fig. 1.
The organizations of Korea Occupational Disease Surveillance.
The Department of OEM at the university hospital, designated as the center, will work
in collaboration with the MOEL regional office to establish a coordination system.
This system will involve various hospitals within the region and will integrate with
the emergency medical system and other clinical departments of the hospital. The aim
is to facilitate the reporting of various suspected cases of occupational diseases
identified in the region. Each center compiles these reports and submits them to the
MOEL, allowing for a national overview of the data. Data concerning monitored cases
of occupational diseases are communicated to the MOEL and the Korea Occupational
Safety and Health Agency. Some of these reported cases may undergo further testing
for confirmation. If necessary, preventive measures may be developed in
collaboration with the MOEL and the Korea Occupational Health and Safety Agency.
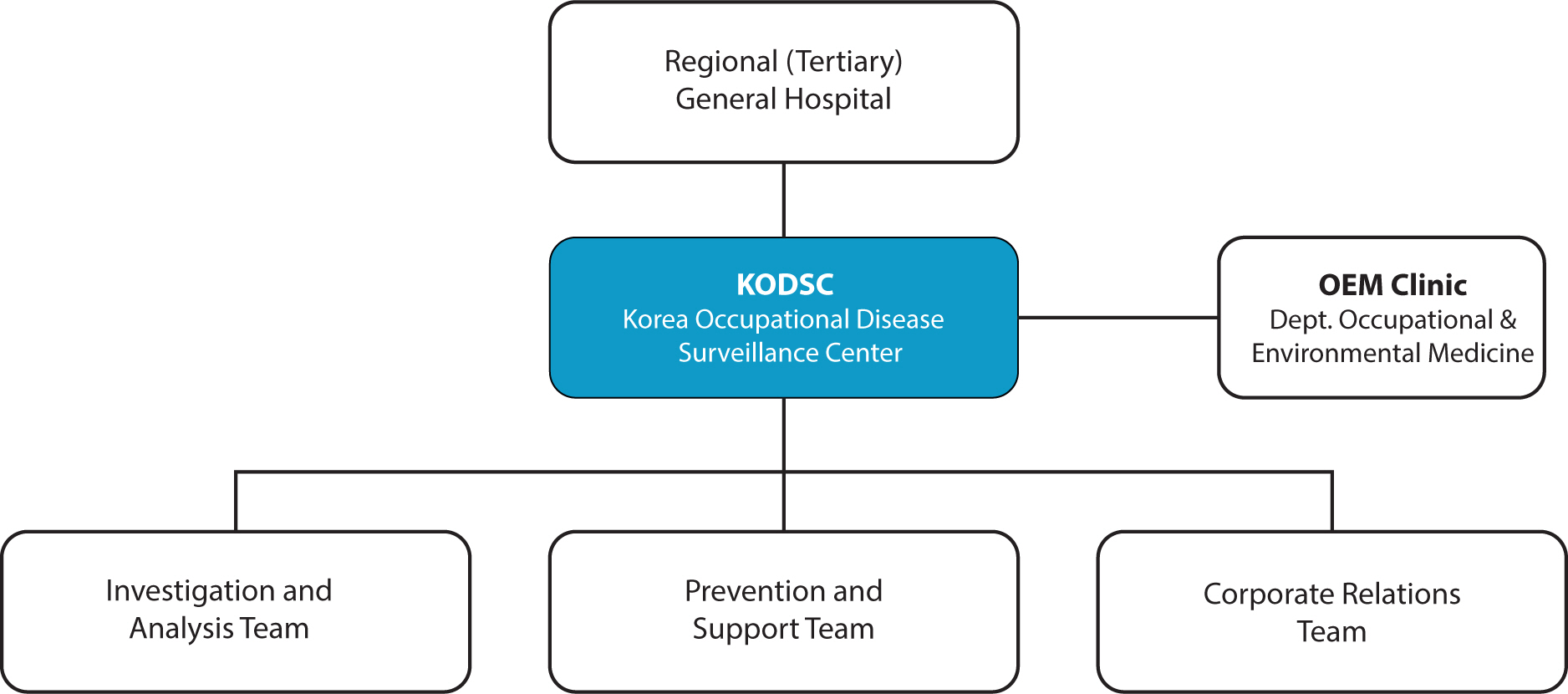
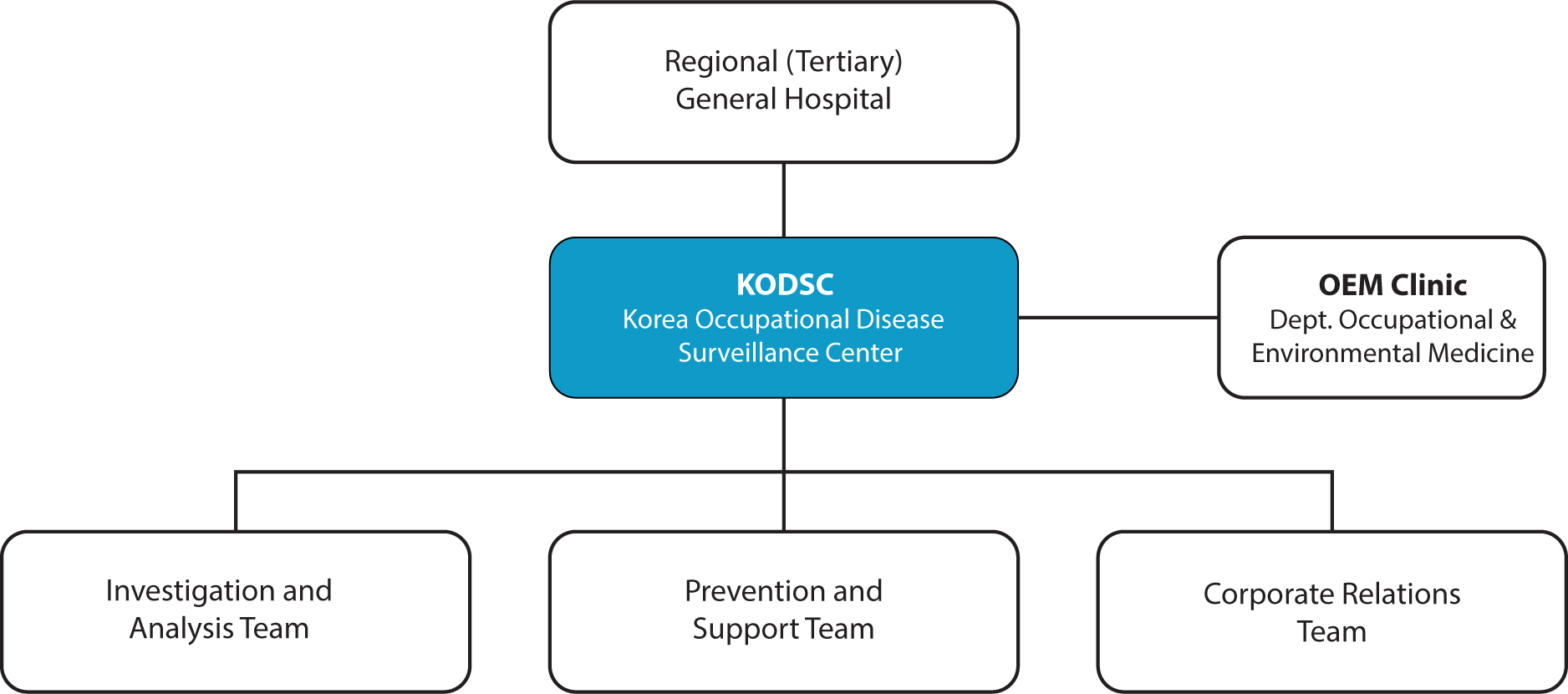
Fig. 2 illustrates the roles and
responsibilities of the center, which is divided into three teams: the Investigation
and Analysis Team (IAT), the Prevention and Support Team (PST), and the Corporate
Relations Team (CRT). Each center includes occupational and environmental clinics
that diagnose and treat patients with occupational diseases. The IAT manages the
KODSC, which initially collects patient information when a suspected occupational
disease is reported. This team also determines whether a risk investigation is
necessary. If so, the IAT coordinates an on-site investigation at the workplace
where the disease was reported. The primary role of the IAT is to assess the
work-relatedness of the disease in patients with suspected occupational diseases and
to manage data on these cases. Doctors and health professionals in emergency rooms
or clinics may encounter patients suspected of having occupational diseases. In such
instances, they can report these cases to the KODSC without a confirmatory test.
They simply complete a prespecified form and submit it via a homepage, SMS, social
network service, or health information system. Most reported cases are stored in the
database after evaluation and clarification by the OEM doctors and health
professionals at the KODSC.
Fig. 2.
The organization of each Korea Occupational Disease Surveillance
Center.
In cases requiring urgent intervention, the KODSC collaborates with MOEL and KOSHA to
support occupational disease investigations. This includes conducting workplace
inspections and walk-through surveys to identify occupational hazards. PST supports
the IAT in executing on-site workplace investigations. Working closely with KOSHA,
the team visits sites where severe occupational diseases have been reported or are
likely to occur, offering consultation and recommendations for improvements. For
instance, after an on-site investigation, the team may conduct sample analyses of
suspect chemicals, such as cleaning agents, either independently or in cooperation
with KOSHA. Following the investigation, in conjunction with KOSHA, the team
provides details on the workplace environmental improvement support scheme.
Additionally, if necessary, they offer information on workers’ compensation
procedures to patients with occupational diseases.
The CRT is responsible for maintaining and managing a network designed to collect
reports of suspected occupational diseases. The team strives to ensure the network
remains fully operational to handle incoming cases. It collaborates with the
emergency department coordinator to confirm the medical histories of patients
visiting the emergency department. Additionally, the CRT routinely visits partner
hospitals and other relevant institutions within the region to gather data on
suspected occupational disease cases, which are then forwarded to the IAT. This
process forms the foundation of the national occupational disease database. However,
significant cases and outbreaks necessitate immediate action. Establishing a network
through connections with local medical staff is crucial. Moreover, maintaining a
strong relationship with the MOEL and KOSHA is essential. To achieve these goals, we
consistently engage in various activities, including publishing newsletters and
organizing workshops.
Korea Occupational Disease Surveillance Center statistics
The case definitions for reporting included occupational diseases caused by physical,
chemical, and biological factors, with the exception of cases involving evident
trauma. There was a particular emphasis on reporting suspected cases of acute
poisoning in relation to the Serious Accident Punishment Act (SAPA). Work-related
musculoskeletal disorders, which represent the majority of workers'
compensation claims, are not required to be reported. Additionally, cerebrovascular
or cardiovascular disorders that have already been diagnosed and are known are also
excluded from reporting. As a general rule, all occupational diseases must be
reported, regardless of the patient's nationality or whether they are
enrolled in a worker’s compensation insurance scheme.
Table 2 displays the number of suspected cases
reported since the establishment of the KODSC in 2023. That year, a total of 4,341
suspected cases were reported nationwide, with 57 cases receiving assistance for
investigations under the SAPA. About 30% of these cases were reported through
outpatient services or admissions at hospitals operating their own KODSC. Meanwhile,
approximately 39% of the cases were reported by partner hospitals participating in
the network.
Table 2.
Reported cases in 2023
Suspicious case reports
Investigation
Total
KODSC OPD or Adm
KODSC ER
Partner hospital
Others
Total
Risk investigation
Investigation support
1,306
509
1,700
826
4,341
24
33
4,389
(30.1%)
(11.7%)
(39.2%)
(19.0%)
(100.0%)
KODSC, Korea Occupational Disease Surveillance Center.
In relation to the total number of reports, organic chemicals emerged as the most
common risk factor associated with these health issues, comprising 20.5% of the
cases. This was followed by mineral dust, which accounted for 12.9%. Subsequent risk
factors included biological elements such as gases, metals, acids, and alkalis.
Welding fumes were suspected as the causative agent in 3.5% of the incidents. In
5.3% of the cases, identifying a probable risk factor was not feasible due to
privacy or consent limitations during the reporting process, which hindered further
investigation of the workplace (Table 3).
Table 3.
Suspected risk factors for reported cases in 2023
Risk factors
Number (%)
Organic chemicals
888 (20.5)
Mineral dusts
560 (12.9)
Biological factors
349 (8.0)
Gases
316 (7.3)
Metals
284 (6.5)
Acids or alkalis
256 (5.9)
Asbestos
214 (4.9)
Ultraviolet
214 (4.9)
High temperature
178 (4.1)
Welding fume
154 (3.5)
Hypoxia
92 (2.1)
Wood dust
58 (1.3)
Metalworking fluids
40 (0.9)
Man-made fibers (glass fibers)
13 (0.3)
Ionizing radiation
6 (0.1)
Abnormal barometric pressure
3 (0.1)
Others
484 (11.1)
Unknown
232 (5.3)
Total
4,341 (100)
The most commonly reported condition was "Injuries involving multiple body
regions, poisoning, other traumas," which includes acute poisoning, the
primary focus of the surveillance system, accounting for 28.6% of all reports.
Respiratory diseases were present in 23.8% of the cases, and cancer was reported in
301 cases (Table 4). Considering that
workers' compensation recognizes only about 500 chemical exposure-related
illnesses annually, the surveillance system captures a broader spectrum of milder
illnesses, complicating direct comparisons. Nevertheless, it proves effective in
uncovering the broader scope of issues beneath the surface.
Table 4.
Disease classifications of reported cases in 2023
Disease classification
Number (%)
A
Infection
46 (1.1)
B
Virus or parasite
76 (1.8)
C
Malignant neoplasm
301 (6.9)
D
Benign neoplasm, hematologic or
immune
34 (0.8)
E
Endocrine, nutritional and metabolic
6 (0.1)
F
Mental and behavioral
4 (0.1)
G
Nervous system
32 (0.7)
H
Eye and adnexa, ear and mastoid
process
374 (8.6)
I
Circulatory system
76 (1.8)
J
Respiratory system
1,034 (23.8)
K
Digestive system
26 (0.6)
L
Skin and subcutaneous tissue
259 (6)
M
Musculoskeletal system and connective
tissue
21 (0.5)
N
Genitourinary system
26 (0.6)
R
Symptoms, signs and abnormal clinical and
laboratory findings
247 (5.7)
S
Injuries
69 (1.6)
T
Injuries involving multiple body regions,
poisoning, other traumas
1,241 (28.6)
U
Codes for special purposes
1 (0)
V
Transport accidents
1 (0)
W
Other external causes of accidental
injury
9 (0.2)
X
High temperature
272 (6.3)
Y
Event of undetermined intent
1 (0)
Z
Factors influencing health status and
contact with health services
110 (2.5)
Unknown
75 (1.7)
Total
4,341 (100)
Some reported cases were sentinel cases of high public health importance that
urgently required government intervention. For example, in Seoul, a case of toxic
hepatitis linked to trichloromethane in a cleaning product was reported. Following
confirmation of this case, an ad hoc medical examination of all workers using the
product identified six additional cases of toxic hepatitis. In Gwangju, a case of
blood cancer potentially caused by benzene exposure prompted a thorough assessment
of workplace conditions and biological monitoring of the workers. Lastly, in Daegu,
a reported case of acute arsine poisoning, along with several other serious
illnesses in the workplace, initiated an investigation into provisional medical
examinations and compliance with relevant laws and regulations.
Conclusion
More workers are being approved for compensation for work-related illnesses because
the workforce is aging and various occupational factors exacerbate workers’
health problems. Workers engaged in multiple or short-term, precarious jobs are
particularly vulnerable to acute poisoning, especially if they lack familiarity with
their work environments or the chemicals they handle. There is a growing academic
and policy focus on socio-psychological risk factors, such as work hours and stress
[25]. However, due to shifts in the labor
market, health issues are increasingly being examined in sectors with a high
concentration of vulnerable workers, such as construction [26] and gig labor [27].
The labor market's increasing polarization and flexibility have resulted in a
diverse group of workers who fall outside the protection of the current occupational
health system and workers' compensation insurance. Consequently, implementing
full-time surveillance systems in hospitals has become a crucial policy tool [28].
The KODSC is a regional hospital-based surveillance system designed to detect
occupational diseases, including acute poisoning. Established in April 2022, it
builds on the experiences of various surveillance systems in Korea. Despite its
recent inception, the KODSC has successfully identified previously unrecognized
occupational diseases of varying severity. It specifically addresses cases of acute
poisoning that necessitate immediate intervention in the workplace and contributes
to the establishment of national prevention policies through prompt action.
The foundational structure for strengthening the promotion and delivery of
occupational health services involves collecting, analyzing, and disseminating data
on workers' health at the national level [29]. In this context, the KODSC plays a crucial role as it is a publicly
funded, hospital-based system that allows the government to continuously monitor
various occupational diseases. Utilizing the KODSC, data on occupational diseases
can be generated to aid in the planning and implementation of policies. This enables
us to address critical questions like, 'What is the most important and urgent
problem?' Addressing this question is the initial step in resolving public
health issues.
Authors' contributions
Project administration: Jang TW, Chung I, Kim HC, Park J, Kim J, Jeong KS, Kim Y,
Lee CG, Kim H, Song J
Conceptualization: Lee DW, Kim I
Methodology & data curation: Hwang J, Choi S, Kim Y, Lee ES, Hyeoncheol
Oh, Min J
Funding acquisition: Kim I
Writing – original draft: Lee DW, Kim I
Writing – review & editing: Lee DW, Kim I, Hwang J, Choi S, Jang
TW, Chung I, Kim HC, Park J, Kim J, Jeong KS, Kim Y, Lee ES, Kim Y, Jeong I,
Hyunjeong Oh, Hyeoncheol Oh, Ha JC, Min J, Lee CG, Kim H, Song J
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This research was supported by Ministry of Employment and Labor, Republic of
Korea.
Data availability
The data are available upon request.
Acknowledgments
Not applicable.
Supplementary materials
Not applicable.
References
1. Kang SK, Kim EA. Occupational diseases in Korea. J Korean Med Sci 2010;25(Suppl):S4-S12.
3. Japan Industrial Safety & Health
Association. Fatal occupational injuries per 100'000 workers in ILOSTAT
(2012-2022) [Internet]. Tokyo (JP): Japan Industrial Safety & Health
Association; c2024 [cited 2024 Nov 10]. Available from: https://www.jisha.or.jp/english/statistics/202310_38.html
10. Smith PF, Hadler JL, Stanbury M, Rolfs RT, Hopkins RS. “Blueprint version 2.0”: updating public health
surveillance for the 21st century. J Public Health Manag Pract 2013;19(3):231-239.
11. Choi SB, Lee S, Lee W. Status and prediction of disapproval of the Korean
workers' compensation insurance for diseases and
injuries. J Occup Health 2023;65(1):e12392.
13. Kang SK, Jee YK, Ahn YS, Kim HO, Ha MN, Kwon HJ, et al. The present status and perspective of nationwide occupational
diseases surveillance system. Korean J Occup Environ Med 2001;13(2):116-126.
15. Ryu J, Lim KH, Ryu DR, Lee HW, Yun JY, Kim SW, et al. Two cases of methyl alcohol intoxication by sub-chronic
inhalation and dermal exposure during aluminum CNC cutting in a small-sized
subcontracted factory. Ann Occup Environ Med 2016;28(4):65
16. Do SY, Lee CG, Kim JY, Moon YH, Kim MS, Bae IH, et al. Cases of acute mercury poisoning by mercury vapor exposure during
the demolition of a fluorescent lamp factory. Ann Occup Environ Med 2017;29(2):19
17. Shin MY, Park JS, Park HD, Lee J. HCFC-123-induced toxic hepatitis and death at a Korean fire
extinguisher manufacturing facility: a case series. Ann Occup Environ Med 2018;30(1):20
18. Hwang JH, Kim JI. A case report of toxic hepatitis caused by chloroform in
automotive parts manufacturer coating process. Ann Occup Environ Med 2022;34:e22.
19. Kwon SC, Song J, Kim Y, Calvert GM. Work-related asthma in Korea - findings from the Korea
work-related asthma surveillance (KOWAS) program, 2004-2009. Allergy Asthma Immunol Res 2015;7(1):51-59.
20. Leem JH, Kim HC, Ryu JS, Won JU, Moon JD, Kim YC, et al. Occupational lung cancer surveillance in South Korea,
2006-2009. Saf Health Work 2010;1(2):134-139.
21. Koh DH, Park JH, Lee SG, Kim HC, Choi S, Jung H, et al. Development of Korean CARcinogen EXposure: an initiative of the
occupational carcinogen surveillance system in Korea. Ann Work Expo Health 2021;65(5):528-538.
22. Min YS, Lee S, Kim M, Ahn YS. Rheumatoid arthritis in low-level toluene-exposed workers based
on nationwide medical surveillance data in Korea. Am J Ind Med 2021;64(4):245-250.
23. Min YS, Ahn YS. Central nervous system diseases of organic solvents exposed
workers based on nationwide medical surveillance-data in
Korea. Am J Ind Med 2016;59(5):392-398.
24. Rutstein DD, Mullan RJ, Frazier TM, Halperin WE, Melius JM, Sestito JP. Sentinel health events (occupational): a basis for physician
recognition and public health surveillance. Am J Public Health 1983;73(9):1054-1062.
25. Kang HT, Kim CJ, Lee DW, Park SG, Lee J, Youn K, et al. Statement by the Korean Society of Occupational and Environmental
Medicine on the proposed reform of working hours in South
Korea. Ann Occup Environ Med 2023;35:e17.
26. Lee S, Kim YJ, Kim Y, Kang D, Kim SC, Kim SY. Incidence rates of injury, musculoskeletal, skin, pulmonary and
chronic diseases among construction workers by classification of occupations
in South Korea: a 1,027 subject-based cohort of the Korean Construction
Worker's Cohort (KCWC). Ann Occup Environ Med 2023;35:e26.
27. Kim MS, Oh J, Sim J, Yun BY, Yoon JH. Association between exposure to violence, job stress and
depressive symptoms among gig economy workers in Korea. Ann Occup Environ Med 2023;35:e43.
28. Yang L, Branscum A, Kincl L. Understanding occupational safety and health surveillance: expert
consensus on components, attributes and example measures for an evaluation
framework. BMC Public Health 2022;22(1):498
Firefighters’ Exposures to Contaminants and Adverse Impacts on Their Health: Why the UK Needs Better Occupational Disease Recognition for Firefighters Along Global Lines, Better Occupational Health Services, and Improved Health Surveillance Andrew Watterson, Rory O’Neill Occupational Health.2026; 1(1): 8. CrossRef
Work-Related Asthma: An Occupational Medicine Perspective Yangwoo Kim, Inah Kim, Jaechul Song Allergy, Asthma & Immunology Research.2026; 18(3): 323. CrossRef
Biological Monitoring as a Preventive Occupational Healthcare Tool: Urinary Biomarkers of Benzene and Toluene Exposure Among Small-Scale Printing Workers in South Korea Jungho Hwang, Yangwoo Kim, Inah Kim, Seoyeon Kim, Juyeoung Hwang, Hyein Park, Ki-Youn Kim Healthcare.2026; 14(13): 1856. CrossRef
Occupational Toxic Effect Episodes in a University Hospital, 2021–2024: A Descriptive Analysis Within the Korean Occupational Disease Surveillance Center Yangwoo Kim, Ha-Eun Lee, Jei Kim, Tae-Won Jang Safety and Health at Work.2025; 16(4): 438. CrossRef
Occupational and Environmental Health Screening Cohort of Yangsan Korea (OEC-YK): 2012–2023 Dongmug Kang, Eun-Soo Lee, Se-Yeong Kim, Youngki Kim, Youn Hyang Lee, Yoon-Ji Kim Annals of Occupational and Environmental Medicine.2025; 37: e32. CrossRef

 , Inah Kim3,4,*
, Inah Kim3,4,*