Abstract
Elastofibroma dorsi is a rare, benign soft tissue tumor that typically arises in the infrascapular region. Although it is often asymptomatic, some patients experience pain or a snapping sensation during shoulder movement, which warrants surgical excision. We report a symptomatic case in a middle-aged male patient, highlighting the diagnostic imaging features and surgical management of this condition.
-
Keywords: Elastofibroma dorsi; Infrascapular soft tissue tumor; Shoulder pain; Case reports
Introduction
Background
Elastofibroma dorsi is an uncommon, slow-growing benign soft tissue neoplasm that is predominantly located in the infrascapular region and is histologically characterized by the proliferation of collagenous and elastic fibers interspersed with adipose tissue. It primarily affects older adults and demonstrates a marked female predominance [
1]. Although elastofibroma dorsi is frequently asymptomatic, some patients experience pain or discomfort, particularly during shoulder movement, which represents a characteristic clinical manifestation of the lesion [
2].
The diagnosis of elastofibroma dorsi is primarily based on clinical findings and characteristic imaging features. Ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) are commonly used. Ultrasonography typically demonstrates a pattern of alternating hyperechoic and hypoechoic linear areas beneath the scapula. CT reveals a well-demarcated lesion containing areas of fat attenuation that are usually less dense than adjacent muscle. MRI provides superior diagnostic accuracy, demonstrating a heterogeneous soft tissue mass with interspersed fatty streaks. Biopsy is rarely required unless imaging findings are atypical or there is evidence of rapid lesion growth [
3].
Although elastofibroma dorsi typically presents with characteristic clinical and imaging findings, its underlying pathogenesis remains incompletely understood. Several hypotheses have been proposed, with one widely accepted theory suggesting that repetitive mechanical stress between the scapula and the thoracic wall contributes to lesion development. In addition, a possible hereditary predisposition and abnormalities in elastic fiber formation have been proposed as contributing factors [
4].
The management of elastofibroma dorsi is guided by the presence and severity of clinical symptoms. In asymptomatic cases, which are often detected incidentally, active treatment is not required, and periodic observation is sufficient. When the lesion causes discomfort or restricts shoulder movement, surgical excision is generally recommended. Complete excision typically results in symptom resolution, with a low risk of recurrence and minimal postoperative complications, such as seroma formation [
5]. Given the benign nature of elastofibroma dorsi, marginal excision with minimal removal of surrounding healthy tissue is considered adequate and is associated with low recurrence and complication rates [
6].
This case report describes a symptomatic case of elastofibroma dorsi in a middle-aged male patient, with emphasis on clinical presentation, radiological diagnosis, and surgical management.
Case presentation
Ethics statement
Written informed consent was obtained from the patient for publication of this case report and the accompanying images.
Patient information
A 51-year-old male patient presented with a 2-month history of right shoulder discomfort accompanied by a clicking sensation during arm abduction. The patient had no significant past medical history. He reported frequent occupational and recreational use of the right shoulder, which may have contributed to repetitive mechanical stress, a factor often implicated in the development of elastofibroma dorsi.
Clinical findings
Physical examination revealed a non-tender, mobile, firm mass in the right infrascapular region (
Fig. 1). A distinct clicking sound was elicited during active shoulder movement.
Ultrasonography demonstrated a heterogeneous, hypoechoic lesion with poorly defined margins located beneath the latissimus dorsi muscle, without evidence of internal vascularity. MRI revealed a well-circumscribed soft tissue mass measuring 7×2×7 cm, located between the inferior border of the scapula and the chest wall, deep to the latissimus dorsi muscle. The lesion exhibited a characteristic combination of fibrous and fatty components, producing a layered or striated appearance on both T1- and T2-weighted images, without evidence of invasion into adjacent structures. Based on the clinical presentation and characteristic radiological features, elastofibroma dorsi was considered the most likely diagnosis. Given the symptomatic nature of the lesion, surgical excision was recommended.
Therapeutic intervention
The patient subsequently underwent surgical excision under general anesthesia. A posterior approach was used, and the patient was placed in the prone position to optimize access to the infrascapular region. Careful dissection was performed through the fibers of the latissimus dorsi muscle to expose the lesion (
Fig. 2). During dissection, elevating the arm to approximately 90°–120° with slight anterior angulation helped shift the scapula laterally and loosen the underlying tissue. This maneuver brought the lesion into a more superficial plane, thereby improving visibility and facilitating surgical access. As a result, exposure was enhanced, the need for extensive deep dissection was reduced, and lesion handling became easier and safer. Although the tumor lacked a distinct capsule, it was well demarcated from the surrounding tissues and was removed en bloc (
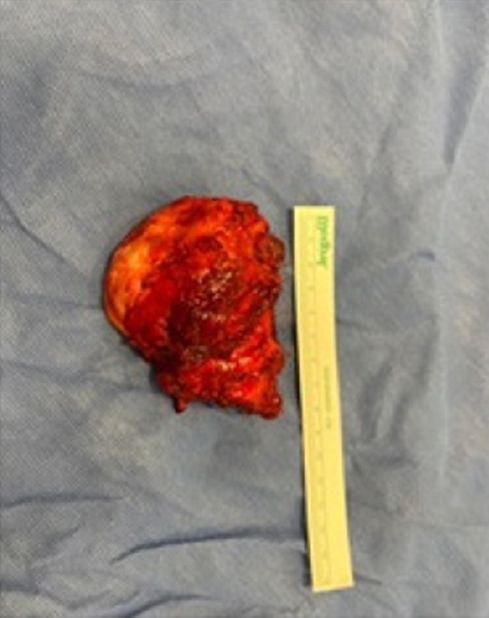
Fig. 3). Intraoperatively, the lesion had a firm, rubbery consistency, consistent with previous descriptions of elastofibroma dorsi. Hemostasis was achieved meticulously, and the surgical site was closed in layers. A suction drain was placed to minimize postoperative seroma or hematoma formation, which are common complications related to the lesion’s deep location and size.
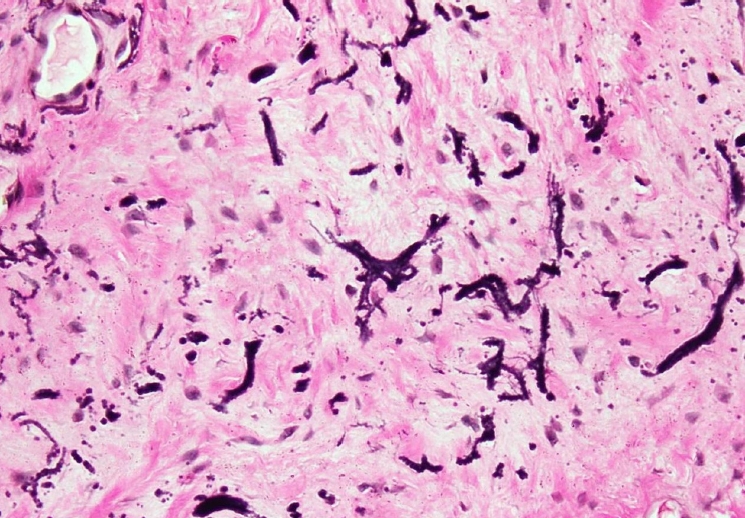
Histopathological examination of the excised lesion revealed dense collagenous stroma interspersed with abnormal elastic fibers and mature adipose tissue, consistent with elastofibroma dorsi. No cellular atypia or features suggestive of malignancy were identified. These findings confirmed the presumptive diagnosis based on the clinical and radiological assessment (
Fig. 4).
The postoperative course was uneventful, and the patient was discharged on postoperative day 3. At the 2-week follow-up visit, the incision had healed satisfactorily (
Fig. 5), and the patient reported marked symptomatic improvement, including resolution of the clicking sensation and improvement in shoulder range of motion.
Discussion
Elastofibroma dorsi is an uncommon benign soft tissue tumor that predominantly affects older adults, and several studies have reported a higher prevalence in females than in males [
5-
7]. Although most cases are unilateral, bilateral involvement has also been described, albeit less frequently. However, because comprehensive meta-analyses directly comparing these patterns are lacking, definitive conclusions regarding their relative prevalence remain limited [
8,
9]. Elastofibroma dorsi is often asymptomatic and is discovered incidentally, but it may become clinically apparent when symptoms such as scapular snapping, localized swelling, or discomfort during shoulder movement develop. Although the pathogenesis of elastofibroma dorsi remains incompletely understood, repetitive mechanical friction between the scapula and thoracic wall has been widely proposed as a factor that contributes to lesion development via degenerative changes in the connective tissues [
10]. Histologically, the tumor is composed of dense collagenous stroma interspersed with abnormal elastic fibers and variable amounts of mature adipose tissue. This histological architecture closely corresponds to its characteristic radiological appearance and helps distinguish it from malignant soft tissue neoplasms [
11]. Radiological evaluation plays a central role in the diagnosis of elastofibroma dorsi. Ultrasonography often demonstrates a poorly defined, heterogeneous, hypoechoic lesion with minimal or absent internal vascularity. However, because ultrasonography is operator-dependent and may be less accurate in differentiating deep infrascapular soft tissue tumors, MRI is generally preferred for precise characterization. MRI remains the imaging modality of choice and typically reveals a well-circumscribed mass with alternating fibrous and fatty layers. This appearance produces the characteristic striped or speckled pattern on T1- and T2-weighted images, which supports the diagnosis. Although MRI findings are highly suggestive, they are not entirely pathognomonic. Lesions such as desmoid-type fibromatosis, fibroma, or low-grade soft tissue sarcoma may show partially overlapping imaging features. Furthermore, as in our case, the lesion’s location beneath the latissimus dorsi and adjacent to the inferior scapular margin supports the diagnosis and may reduce the need for invasive diagnostic procedures.
In our patient, right shoulder discomfort and a characteristic clicking sound prompted further imaging evaluation. Ultrasonography demonstrated a heterogeneous hypoechoic lesion; however, because of the lesion’s depth and the operator-dependent nature of ultrasonography, MRI was performed for more precise assessment.
Although elastofibroma dorsi is benign and slow growing, surgical resection is often indicated in symptomatic patients, particularly when pain, mechanical irritation, or shoulder dysfunction interferes with daily activities. Surgery may also be considered when imaging findings are inconclusive or when there is concern for malignancy. Complete surgical excision is typically curative, and reported recurrence rates are low. The literature supports operative treatment in appropriately selected patients and indicates excellent postoperative outcomes. Postoperative recovery is generally uneventful. Nevertheless, because of the lesion’s deep anatomical location and relatively large size, complications such as seroma or hematoma formation may occur. These complications are usually minor and can be effectively managed with meticulous intraoperative hemostasis and placement of suction drains to reduce fluid accumulation.
Although elastofibroma dorsi is generally more prevalent in females, our case involved a male patient. Consistent with previous reports, the patient presented with pain and a characteristic clicking sensation. Following surgical treatment, his symptoms resolved completely. This outcome further supports the effectiveness of surgery in symptomatic patients.
This case illustrates the clinical, radiological, and surgical management of elastofibroma dorsi in a symptomatic male patient. It also highlights practical considerations in operative planning and provides useful insights for clinicians managing similar lesions.
-
Authors’ contribution
Conceptualization: ŞK, MSA. Data curation: ŞK, GÖ, OÖ, CK. Methodology/formal analysis/validation: ŞK, MSA, HCÇ, MK, OD. Project administration: ŞK, MSA, GÖ, OÖ. Writing–original draft: ŞK. Writing–review & editing: MSA.
-
Conflict of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Fig. 1.Mobile soft tissue mass in the right infrascapular region. The lesion becomes more prominent with shoulder abduction. Written informed consent for the publication of this image was obtained from the patient.

Fig. 2.Intraoperative image after dissection of the latissimus dorsi muscle, exposing the elastofibroma dorsi lesion. Written informed consent for the publication of this image was obtained from the patient.

Fig. 3.Macroscopic view of the resected elastofibroma dorsi. The lesion appears as a well-defined, firm, gray-white mass with characteristic fibrous and elastic tissue components.
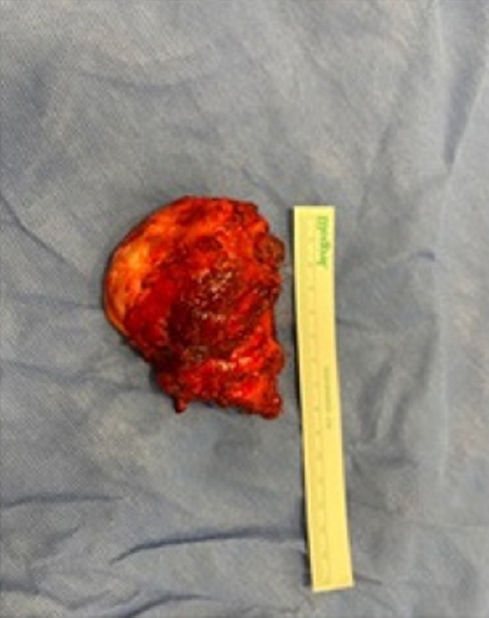
Fig. 4.Histopathological section of the excised lesion demonstrating dense collagenous stroma with interspersed, coarse, wavy elastic fibers. The general tissue architecture is shown with hematoxylin and eosin (H&E) stain, while elastic fibers are highlighted using Verhoeff–Van Gieson (VVG) stain, consistent with elastofibroma dorsi (original magnification ×10).
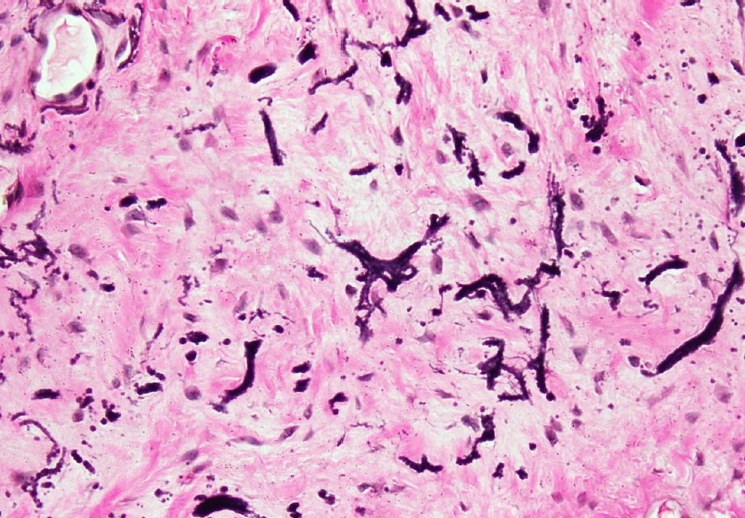
Fig. 5.Postoperative wound at 2 weeks, demonstrating satisfactory healing with no signs of infection, dehiscence, or hypertrophic scarring. Written informed consent for the publication of this image was obtained from the patient.

References
- 1. Järvi OH, Saxén AE, Hopsu-Havu VK, Wartiovaara JJ, Vaissalo VT. Elastofibroma: a degenerative pseudotumor. Cancer 1969;23:42-63. https://doi.org/10.1002/1097-0142(196901)23:1<42::aid-cncr2820230105>3.0.co;2-#
- 2. Bedirhan MA, Sağay SS, Cansever L, Kocatürk C, Yalçınkaya İ. Elastofibroma dorsi: a review of 42 cases. Turk Gogus Kalp Damar Cerrahisi Derg 2014;22:126-128. https://doi.org/10.5606/tgkdc.dergisi.2014.8276
- 3. Bartocci M, Dell'Atti C, Meacci E, Congedo MT, Magarelli N, Bonomo L, Leone A. Clinical features, imaging findings, treatment aspects of elastofibroma dorsi and long-term outcomes after surgical resection. Eur Rev Med Pharmacol Sci 2017;21:2061-2068.
- 4. Mardani P, Kamran H, Ayare N, Shahriarirad R, Shahabinejad P, Geramizadeh B, Vafabin M. Subscapular elastofibrolipoma treated with marginal resection: two case reports. J Med Case Rep 2022;16:296. https://doi.org/10.1186/s13256-022-03522-4
- 5. Karakurt O, Kaplan T, Gunal N, Gulbahar G, Kocer B, Han S, Dural K, Sakinci U. Elastofibroma dorsi management and outcomes: review of 16 cases. Interact Cardiovasc Thorac Surg 2014;18:197-201. https://doi.org/10.1093/icvts/ivt442
- 6. Scamporlino A, Ruggiero C, Aramini B, Morandi U, Stefani A. Surgery for elastofibroma dorsi: optimizing the management of a benign tumor-an analysis of 70 cases. J Thorac Dis 2020;12:1884-1894. https://doi.org/10.21037/jtd-20-649
- 7. Deveci MA, Özbarlas HS, Erdoğan KE, Biçer ÖS, Tekin M, Özkan C. Elastofibroma dorsi: Clinical evaluation of 61 cases and review of the literature. Acta Orthop Traumatol Turc 2017;51:7-11. https://doi.org/10.1016/j.aott.2016.10.001
- 8. Haihua R, Xiaobing W, Jie P, Xinxin H. Retrospective analysis of 73 cases of elastofibroma. Ann R Coll Surg Engl 2020;102:84-93. https://doi.org/10.1308/rcsann.2019.0089
- 9. Gündoğdu E. Elastofibroma dorsi: prevalence and imaging features on multi detector computed tomography. Ankara Eğit Araşt Hast Derg [Internet] 2017 [cited 2025 Dec 20];50:26-31. Available from: https://dergipark.org.tr/en/download/article-file/513877
Figure & Data
Citations
Citations to this article as recorded by


 , Muhammed Said Aydin*
, Muhammed Said Aydin*