초록
프로바이오틱스(probiotics)는 하부 위장관질환의 보조 치료제로서 임상현장에서 점차 주목받고 있다. 그러나 특히 성별 차이에 따른 치료효과를 뒷받침하는 근거는 아직 충분하지 않다. 이 가이드라인은 과민성장증후군, 기능성 변비, 그리고 클로스트리디오이데스 디피실리(Clostridioides difficile) 감염 환자에서 프로바이오틱스 사용에 관한 근거 중심의 고찰과 함께, 성별 차이를 고려한 실용적 권고사항을 제시하고자 한다. 무작위 대조시험 및 메타분석의 근거에 따르면, 프로바이오틱스는 과민성장증후군에서 전반적인 증상, 복통 및 복부 팽만감을 일부 완화하는 효과가 있으며, 기능성 변비에서는 배변 빈도와 대변 굳기를 개선할 수 있다. 다만, 이러한 효과는 균주에 따라 차이가 있고 연구 간 이질성이 크다. 과민성장증후군 관련 임상연구에서는 프로바이오틱스 치료효과에 있어 뚜렷한 성별 차이가 확인되지 않았으나, 스트레스 유발 과민성장증후군 동물모델을 이용한 실험연구에서는 특정 프로바이오틱스 균주에 대한 성별 의존적 반응이 관찰되어, 성별에 따른 반응 차이의 생물학적 타당성을 뒷받침한다. C. difficile 감염의 경우, 1차 감염 및 재발 예방에 대한 프로바이오틱스의 효능은 대규모 연구에서 일관된 결과를 보이지 않으며, 현재 가이드라인에서는 일상적인 사용을 권고하지 않는다. 다만, 면역학적 성별 차이 및 연령에 따른 차이는 C. difficile 감염의 임상 양상 차이를 설명하는 근거가 될 수 있다. 프로바이오틱스는 일반적으로 건강한 성인에서 안전한 것으로 알려져 있으나, 면역 저하자나 중증 환자에게는 신중한 사용이 요구된다. 임상의는 프로바이오틱스 제품을 선택할 때 균주별 임상 근거, 적정 생균 수, 환자의 특성 및 성별 등을 종합적으로 고려하여야 한다. 결론으로, 프로바이오틱스는 과민성장증후군과 기능성 변비의 보조치료로 활용할 수 있으나, 미생물ㆍ숙주ㆍ성별 등 다양한 요인에 따라 치료반응이 달라질 수 있다. 최적화된 맞춤형 프로바이오틱스 치료전략을 확립하기 위해서는 향후 추가적인 연구가 필요하다.
-
Keywords: 클로스트리디오이데스 디피실리(Clostridioides difficile); 변비; 과민성장증후군; 프로바이오틱스; 성
Abstract
Probiotics have gained increasing clinical attention as adjunctive treatment for lower gastrointestinal disorders. However, evidence supporting their therapeutic efficacy remains limited, particularly with regard to sex-related differences. This expert review provides evidence-based insights and practical recommendations for the use of probiotics in patients with irritable bowel syndrome (IBS), functional constipation (FC), and Clostridioides difficile infection (CDI), considering possible sex-related differences. Evidence from randomized controlled trials and meta-analyses indicates that probiotics can modestly improve global symptoms, abdominal pain, and bloating in IBS and enhance bowel movement frequency and stool consistency in FC. However, these effects are strain-specific and heterogeneous. Although clinical studies on probiotics in IBS have not confirmed significant sex-related differences, experimental animal studies using stress-induced IBS models have demonstrated sex-dependent responses to specific probiotic strains, supporting the biological plausibility of such differences. For CDI, the efficacy of probiotics in preventing primary or recurrent infections remains inconsistent across large trials, and current guidelines usually do not recommend their routine use. However, sex- and age-related immunologic differences support the clinical differences of CDI. Probiotics are generally considered safe for healthy individuals, although caution is advised in patients who are immunocompromised or critically ill. Clinicians should select probiotic products based on strain-specific clinical evidence, adequate viable doses, patient characteristics and sex. In conclusion, probiotics might play a role as adjunctive therapy for IBS and FC, with variability in responses influenced by microbial, host, and potential sex-related factors. Further research is needed to establish optimized personalized probiotic strategies.
-
Keywords: Clostridioides difficile; Constipation; Irritable bowel syndrome; Probiotics; Sex
서론
프로바이오틱스(probiotics)는 한 세기 이상 장 건강증진을 위해 발효음료 및 보충제로 널리 섭취되어 왔다. 지난 20년간 장내미생물군에 대한 연구가 급속히 확장되면서, 장내미생물이 인간 건강에 중요한 역할을 한다는 사실이 부각되었고, 이는 프로바이오틱스를 포함한 미생물 기반 치료제의 발전으로 이어졌다. 현재 프로바이오틱스는 과민성장증후군(irritable bowel syndrome, IBS)과 기능성 변비(functional constipation, FC) 같은 하부 위장관질환에 흔히 사용되지만, 클로스트리디오이데스 디피실리 감염(
Clostridioides difficile infection, CDI)에서의 예방적 역할에 대해서 여전히 논란이 많은 측면이 있다[
1-
3]. 또한 기존의 여러 메타분석에도 불구하고, IBS, FC, 또는 CDI에서 증상을 의미 있게 개선하기 위해 필요한 프로바이오틱스 균주, 용량, 투여기간 등에 대해 상당한 불확실성이 남아있어 가장 신뢰할 수 있고 임상적으로 관련성 높은 근거를 바탕으로 심도 있는 고찰이 요구된다. 이러한 연구들 사이의 상당한 차이는 식이부터 생물학적 요인인 성별에 이르는 복잡한 환경요인의 영향에서 기인할 수 있다. IBS와 FC는 여성에게 더 흔하게 발생하며, 장내미생물의 성별 차이가 잘 알려진 점을 고려할 때, 프로바이오틱스는 성별 특이적 치료효과를 나타낼 가능성이 있다. 성호르몬이 특히 면역활동을 통해 장내미생물군에 영향을 미친다는 점은 잘 알려져 있다[
4]. 또한 에스트로젠과 안드로젠 모두 장내미생물군에 의해 영향을 받는데, 특히 폐경기 여성과 노년 남성에서 β-glucuronidase 생성 미생물군에 의한 조절이 두드러진다[
5]. 더 나아가 성별 차이와 장내미생물 구성, 면역 신호전달, 내장감각을 연결하는 생물학적으로 타당한 기전들이 제시되고 있다[
4-
6]. 그러나 프로바이오틱스의 효능이 성별에 따라 다른지에 대한 연구는 거의 없는 실정이다. 이 종설은 프로바이오틱스의 최신 개념을 요약하고, 하부 위장관질환 환자에서의 사용 근거를 성별 관련 차이에 초점을 맞추어 정리하고자 한다.
검색전략 및 문헌 선정
이 종설은 IBS, FC, CDI에 대한 프로바이오틱스의 최신 근거를 성차의 관점에서 요약하고 해석하고자 수행되었다. 문헌검색은 MEDLINE, EMBASE 및 Cochrane Central을 이용하였다. 프로바이오틱스 관련 검색어는 Probiotics,
Saccharomyces,
Lactobacillus,
Bifidobacterium과 관련된 핵심 용어를 조합하여 구성하였다. IBS의 경우, 2023년에 발표된 해당 주제에 관한 최신 체계적 문헌고찰을 핵심 메타분석으로 선정하였다[
7]. 해당 메타분석에 포함된 82건의 임상시험을 개별적으로 검토하였으며, 3개 데이터베이스에서 “irritable bowel syndrome” 또는 “IBS”를 검색어로 조합하여 2023년 1월부터 2025년 4월까지 새로 발표된 연구를 추가로 검색하였다. FC에 대한 프로바이오틱스 효과를 검토하기 위해 2000년 1월부터 2025년 4월까지 “functional constipation,” “constipation,” 및 “FC”를 조합해 상세 검색을 수행했다. CDI에 대한 프로바이오틱스의 효능을 분석하기 위해서는 유사한 검색전략을 사용하여 2000년 1월부터 2025년 8월 사이에 발표된 연구를 검색하였다. CDI 관련 검색어에는 “
Clostridium difficile infection,” “pseudomembranous colitis” 및 “CDI”를 포함하였다. 검색대상은 영어로 발간된 논문으로 제한하였다. 주제와 관련 있는 원저 논문(무작위 대조시험[randomized controlled trial, RCT] 및 관찰연구), 메타분석을 포함한 종설 논문 및 임상 진료지침을 포함하였다. 반면, 증례 보고 및 임상적 관련성이 낮은 연구는 제외하였다. 또한 주요 문헌의 참고문헌 목록을 수동으로 검색(manual screening)하여 추가적인 논문도 확보하였다. 이 논문은 체계적 문헌고찰이 아닌 서술적 종설이므로, 최종 문헌 선정은 임상현장과의 연관성, 연구방법론적 엄격성, 프로바이오틱스의 성별 차이 효과를 이해하는 데 기여하는 정도를 저자들이 질적으로 평가해 결정했다. 결과는 주로 서술적으로 통합했으며, 특정 질환에 미치는 영향, 견해가 일치하거나 논란이 있는 영역, 임상적 함의를 중점적으로 다루었다. 선정된 연구 중 남녀별 결과를 별도로 보고하거나 성별 특이적 하위분석을 제공한 연구를 별도로 분류ㆍ기술하고, 가능할 경우 정량적 통합도 시도하였다.
결과
과민성장증후군 환자에서의 장내미생물 불균형과 프로바이오틱스의 임상적 근거
IBS는 확인 가능한 기질적 위장관질환 없이 복통과 배변 이상을 호소하는 흔한 위장관-뇌 상호작용 장애이다(disorders of brain-gut interaction)[
1]. IBS의 전 세계 유병률은 11.2%로 추정되며, 발생률은 1.35%에서 1.5% 사이이다[
8]. IBS는 특히 성별에 따른 유병률 차이를 보이며, 남성보다 여성에서[
9], 고령층보다 젊은 층에서 더 흔하게 나타난다[
10].
IBS의 병태생리는 아직 부분적으로만 이해되고 있으며[
11], 질환의 장기적인 자연 경과를 변화시키는 것으로 입증된 치료법은 아직 없다. 또한 상당수 환자가 기존 치료에 반응하지 않거나 치료결과에 만족하지 못한다[
12,
13]. 제시된 여러 가설 중에서도 장내미생물의 이상이 IBS의 발생 기전에 깊이 관여하는 것으로 알려지면서[
14,
15], 장내미생물군 조절이 잠재적 치료법으로 부상했다.
프로바이오틱스는 IBS 환자에서 광범위하게 연구되었으며, 증상 완화효과는 수많은 임상시험과 메타분석을 통해 뒷받침되었다[
7,
16-
19]. 비록 기전은 완전히 규명되지 않았고, 단쇄지방산(short chain fatty acid, SCFA) 증가, 염증성 사이토카인 감소, 장벽 기능 개선과 같은 임상 바이오마커는 간접적 표지자(surrogates)에 불과하지만, 프로바이오틱스는 IBS 증상 완화에 도움이 될 수 있다[
20-
22].
2023년 Goodoory 등[
7]이 시행한 메타분석에서는 모든 IBS 아형 환자에서 프로바이오틱스의 효능을 평가했다. 이 분석에는 프로바이오틱스 투여군 1,733명과 대조군 1,636명을 포함한 31건의 RCT가 포함되었다. 메타분석 결과, 높은 이질성에도 불구하고 전반적인 증상(risk ratio [RR], 0.78; 95% confidence interval [CI], 0.71–0.87), 통증(RR, 0.72; 95% CI, 0.64–0.82), 복부 팽만감(RR, 0.75; 95% CI, 0.64–0.88)에서 이점이 있을 가능성을 시사했다.
그러나 균주별 효과는 크게 달랐고, 프로바이오틱스의 균종, 용량, 치료기간, 평가지표 등에서 연구 간 이질성이 컸다.
Escherichia 속 균종들(spp.)은 전반적인 증상 개선에 있어 중등도의 신뢰수준 근거를 보였다.
Lactiplantibacillus plantarum (
Lactobacillus plantarum) 299v를 포함한
Lactobacillus 속 균종들은
Bifidobacterium 속 균종들과 마찬가지로 낮은 신뢰도를 보였으나[
23-
27],
B. infantis 35624는 특정 용량에서 일부 효능을 나타냈다[
28,
29]. 혼합 균주 및
Bacillus 속 또한 낮은 신뢰도를 보였으나, 일부 조합은 제한된 수의 임상시험에서 가능성을 보였다.
Saccharomyces, 특히
S. cerevisiae I-3856 역시 복통 감소에 있어 낮은 신뢰도의 근거와 연관이 있었다. 또한 IBS 아형에 따라 결과를 분석한 연구는 매우 제한적이며, 대부분의 메타분석은 아형에 따른 분석 없이 결과를 보고하였다[
7,
19]. 종합적으로, 이러한 결과들은 뚜렷한 이질성과 균주 특이적 효과로 인해 해석에 주의가 필요하며, 이는 현재의 임상 진료지침에서 균주나 아형에 따른 권고가 없는 원인이 되고 있다[
1,
17,
18,
30].
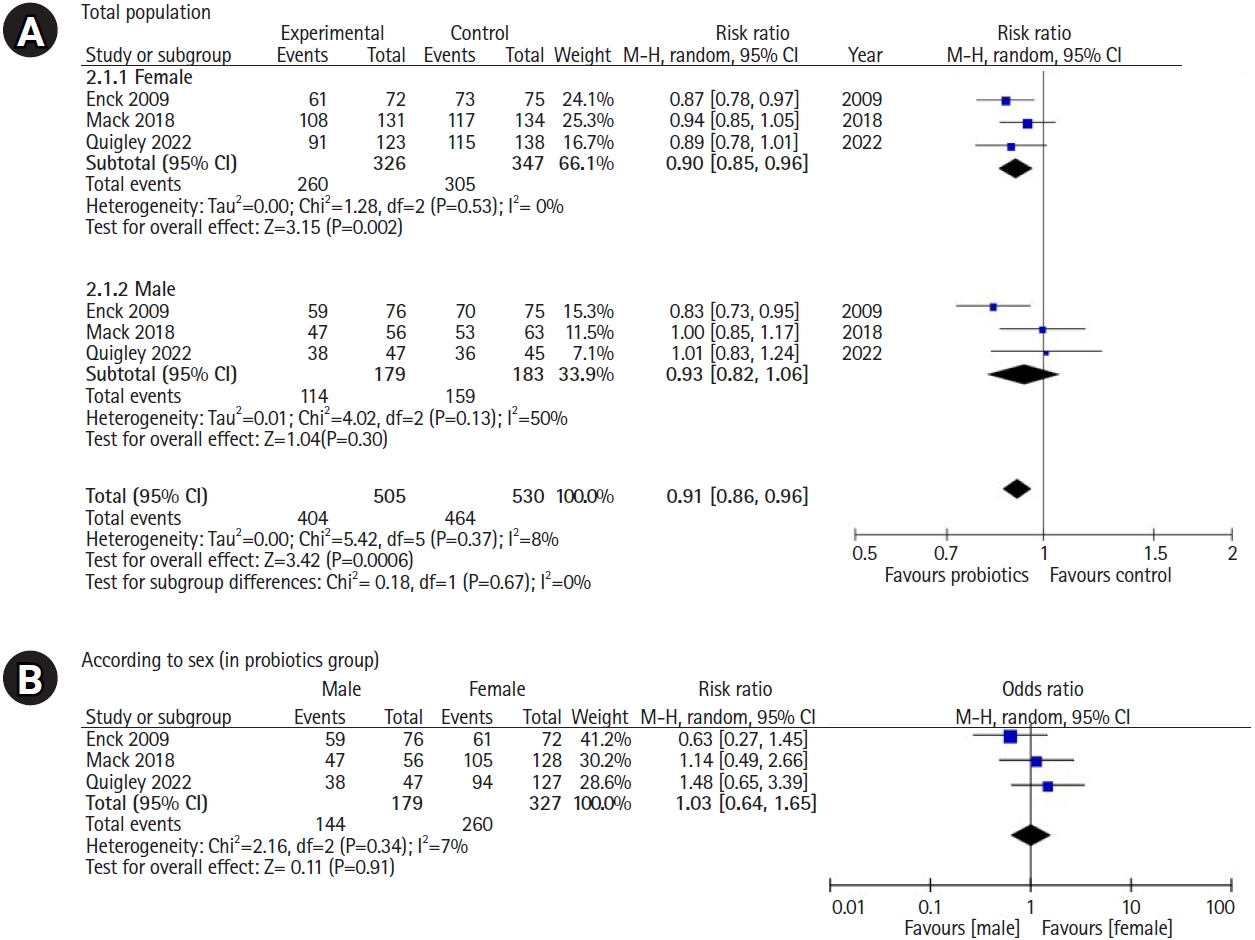
몇몇 IBS 연구에서 프로바이오틱스의 효능을 성별에 따른 치료반응의 차이의 관점으로 보고하였다(
Table 1) [
31-
37]. 최종적으로 3개의 연구가 메타분석에 적합하였으며[
32,
34,
35], 그 결과는
Fig. 1에 제시하였다. 분석결과, 여성 IBS 환자에서 프로바이오틱스의 치료효과가 더 뚜렷하게 나타났으며, 이는 최근 Mullish 등[
38]의 또 다른 연구에 의해 뒷받침되었다. 이 연구에서는 여성 환자에서 IBS 증상 점수가 유의하게 감소하였고, 배변 습관 개선과 더불어 불안, 우울 및 IBS 관련 행동이 감소되었다. 그러나 성별 간의 통계적 유의성에는 도달하지 못하였다. 메타분석에서 개별 종(species) 또는 균주(strain)에 근거한 하위 그룹 분석 또한 불가능하였다. 이러한 결과들은 향후 IBS 치료에 있어 프로바이오틱스 효능의 성별 특이적 차이에 대한 연구의 필요성을 시사한다.
FC 환자에서는 장내미생물 불균형이 관찰되며, 이는
Bifidobacterium spp.,
Lactobacillus spp.,
Prevotella spp. 및 부티르산 생성 속(genera)의 감소와
Coprococcus,
Ruminococcus spp.,
Akkermansia,
Clostridium spp.의 증가를 특징으로 한다[
39,
40]. 변비의 유형에 따라 장내환경과 미생물 구성이 다를 수 있으나, 일반적으로 FC 환자에서는 유익한 젖산 및 부티르산 생성균의 풍부도가 감소하는 반면, 메탄 생성 고균은 증가하는 양상을 보인다[
41]. 반면, 전반적인 미생물 다양성은 연구마다 일치하지 않는데, 이는 IBS나 염증성장질환(inflammatory bowel diseases, IBD) 같은 다른 만성위장관질환에서 전형적으로 다양성이 감소되는 것과는 대조적이다[
42].
프로바이오틱스는 식이섬유 발효를 통해 SCFA를 생성하며, SCFA는 삼투압 효과로 대변량을 증가시키고 장신경계(enteric nervous system)를 자극해 연동운동을 촉진한다[
43]. 특히 SCFA 중 부티르산은 장벽의 무결성(integrity)을 유지하고 세균성 내독소 및 염증반응을 방지하며, 장 운동성 저해를 감소시킨다[
44]. 대장통과시간은 일반적으로 남성보다 여성에서 더 길고[
45], 서행성 변비 또한 여성에게서 더 빈번하게 보고된다. 메탄 생성 미생물의 상대적 풍부도는 서행성 변비 환자에서 유의하게 더 높고, 메탄은 윤상근의 비추진성 수축을 강화하여 연동운동 속도를 지연시킨다[
15,
46]. 일부 프로바이오틱스는 장내미생물 항상성을 회복시키고 메탄 생성균 집단을 감소시킬 수 있다. 이러한 기전들은 프로바이오틱스가 여성 환자에서 더 큰 치료효과를 나타내는 근거가 되는 것으로 보인다.
프로바이오틱스 치료는 장내환경, 상피 면역반응, 장 운동 및 분비활동의 신경내분비적 제어를 조절해 변비증상을 완화하는 다중 기전을 가진다[
47,
48]. 흔히 사용되는 프로바이오틱스는
Bifidobacterium과
Lactobacillus 속의 균종들이지만, FC에 가장 효과적인 균주는 아직 논란이 있다[
49].
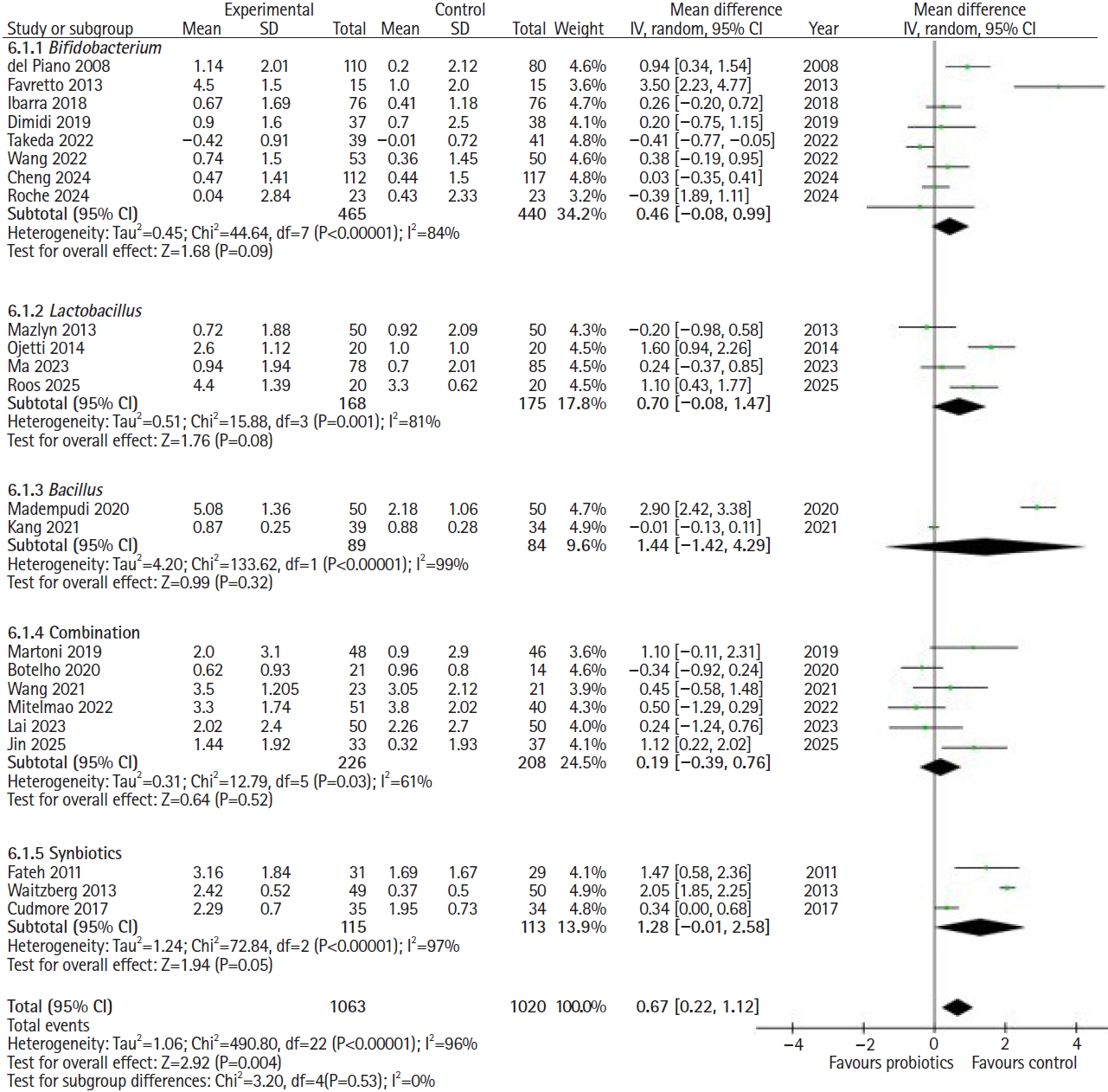
Table 2에 FC 환자에서 프로바이오틱스 효과를 평가한 RCT 25편을 요약하였다[
50-
74]. 다양한 균주와 생균 수(colony forming unit, CFU)를 사용했으며, 각 연구에 포함된 환자 수는 비교적 적었다. 가장 많이 사용된 균주는
Bifidobacterium이며, 그 다음이
Lactobacillus였다. 전반적으로 프로바이오틱스 4주 복용 후 일주일 평균 자발 배변(spontaneous bowel movement, SBM) 횟수가 0.67회(95% CI, 0.22–1.12) 유의하게 증가하였다(
Fig. 2). 그러나 연구 간 이질성은 매우 높았는데(I
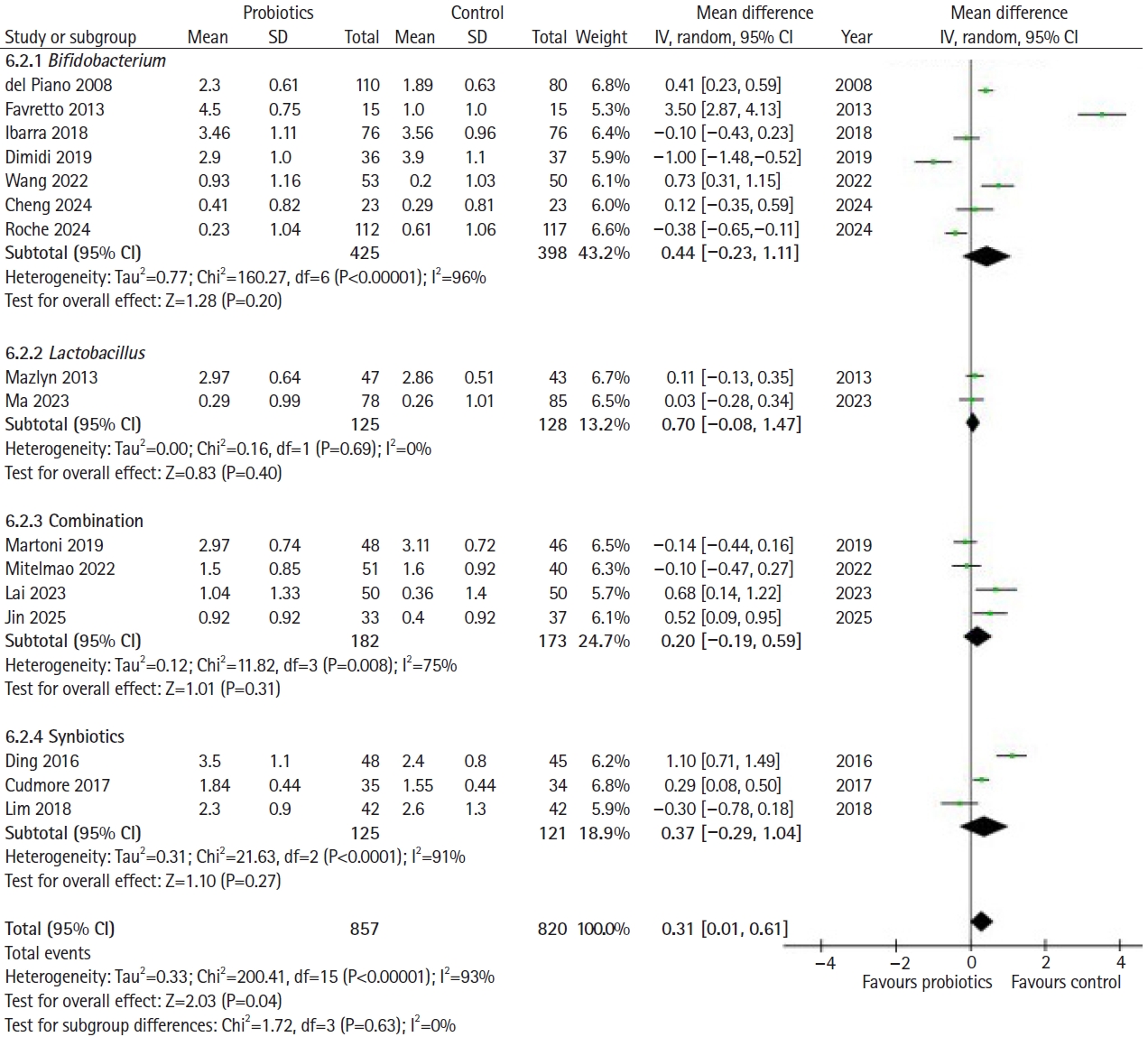
2=96%), 이는 균주, 용량, 증상 중증도, 환자 특성 차이 때문으로 보인다. 균종별 하위 분석결과, 일주일 평균 SBM의 유의미한 증가는 관찰되지 않았으며, 균종 간의 효과 차이 또한 통계적으로 유의하지 않았다. 프로바이오틱스는 4주차에 브리스톨 대변 형태 척도(Bristol stool form scale, BSFS) 점수를 0.31 (95% CI, 0.01–0.61)만큼 약간 개선시켰다(
Fig. 3). SBM 변화와 마찬가지로 균종별 분석에서는 신바이오틱스만 대변의 굳기를 유의하게 개선했다. 일부 연구들이 증상 개선의 가능성을 시사하지만, 이질성과 전반적으로 낮은 근거 수준으로 인해 FC에서 프로바이오틱스의 치료적 가치를 확신하기에는 한계가 있다. 최근 발표된 네트워크 메타분석에서는 균주별로 분류했을 때 어떤 균주도 위약 대비 배변 횟수를 유의하게 증가시키지 못했다[
75]. 이를 자세히 살펴보면, 3건의 연구가 여성 환자만을 대상으로 수행되었다[
52,
54,
74]. Rome III 기준에 따라 진단된 변비 여성 100명을 대상으로 한 연구에서, 매일 6 g의 신바이오틱스(synbiotics,
Lactobacillus 및
Bifidobacterium 종과 프락토올리고당의 혼합물)를 복용한 환자군은 위약군에 비해 더 높은 배변 횟수와 대변 굳기 점수를 기록하였다[
54]. 40명의 여성 변비 환자를 모집한 또 다른 연구에서는
L. gasseri 투여군의 SBM이 5.0±0.9에서 9.4±1.6으로 증가했으나 위약군은 4.2±0.5에서 7.5±0.7회로 증가하는 데 그쳐 의미 있는 차이를 보였다[
74]. 여성만을 대상으로 한 연구들을 분석한 결과, 남녀 모두를 포함한 연구들에 비해 SBM 변화량(주당 2.06회 증가[95% CI, 1.14-2.99])과 대변 굳기 변화량(BSFS 3.5점 증가[95% CI, 2.87-4.13])에서 유의미하게 더 큰 개선효과를 보였다.
CDI는 의료 관련 감염성 설사의 주요 원인으로, 특히 70세 이상에서 전 세계적으로 부담이 증가하고 있다[
76]. CDI 예방에 있어 프로바이오틱스의 예방적 역할을 규명하기 위한 다수의 연구가 수행된 바 있으며(
Supplement 1)[
77-
90], 이 중 대표적 임상시험으로는 1차 예방을 위한 PLACIDE 연구[
79]와 2차 예방을 위한 PICO 연구가 있다[
86]. 그러나 이들 연구는 주로 CDI의 낮은 발생률이나[
79] 군 간 차이가 없어[
86] 유의미한 효과를 입증하는 데 실패하였다. 또한 단일 및 다기관 연구를 포함한 후속 임상연구들에서 그 결과가 일관되게 재현되지 않고 있다[
91,
92].
2017년 코크란 리뷰[
93]와 메타분석[
94]은 프로바이오틱스가 CDI 예방에 유의한 효과가 있음을 보여주었으나, 몇 가지 제한점이 제기되었다. 2017년 코크란 분석에 따르면
Clostridioides difficile 연관 설사 발생률이 60% 감소하였으며, 면역저하자나 중증 쇠약 환자가 아닌 환자에게 항생제와 병용하는 단기 프로바이오틱스 투여는 안전하고 효과적인 것으로 결론지었다[
93]. 그러나 포함된 연구 대부분이 높은 편향 위험을 가졌고, 사후 하위집단 분석결과, 기저 CDI 위험도가 5%를 초과하는 대상군에서만 그 이점이 관찰되었다. 또한 포함된 연구 중 일부에서만 예방효과가 입증되어 결과 해석에 주의를 요한다. 추가적으로 메타분석 과정에서 서로 다른 프로바이오틱스 속을 하나의 범주로 통합함으로써 독특한 생물학적 기전을 가리고 상당한 편향을 초래한다는 제한점도 있다.
이에 따라 여러 가이드라인은 CDI 예방을 위한 프로바이오틱스의 일상적 사용을 권고하지 않고 있다. 그 이유는 첫째, 프로바이오틱스 효능과 비용효과에 대한 명확하고 일관된 근거 부족이다. 앞서 언급한 1차 및 2차 예방 임상시험 모두 유의한 이점을 입증하지 못했다. 둘째, 프로바이오틱스 제품을 둘러싼 상당한 이질성과 불확실성이 주요 쟁점으로 대두되고 있다. 구체적으로는 제품 라벨 정보와의 불일치 및 편차, 균주의 빈번한 오식별ㆍ오분류 또는 생존력 상실, 오염, 그리고 기능적 특성 저하 등이 포함된다[
95]. 이러한 불확실성으로 인해 현재 가이드라인들은 프로바이오틱스의 일상적 사용에 대해 신중하거나[
96], 심지어 반대하는 입장을 취하고 있다[
95,
97]. 또한 안전성 문제도 제기되는데, CDI 위험군에 속하는 환자가 중증 상태이거나 면역이 저하되어 있어 프로바이오틱스 투여가 부적절할 수 있기 때문이다[
95-
97]. 이러한 우려는 항생제 노출 후 프로바이오틱스가 대장의 정상미생물 재정착을 오히려 저해할 수 있음을 시사하는 연구결과들에 의해 더욱 뒷받침된다[
95].
성별 관점에서 여성은 CDI 발생 및 재발률이 높고, 남성은 사망률과 입원기간이 더 길다[
98,
99]. 이는 성별이 질병의 감수성과 예후에 영향을 미칠 수 있음을 시사한다. 최근 데이터는 장내미생물군 구성과 면역체계 등 성별 관련 요인이 역할을 할 수 있음을 보여준다[
100]. 특히 여성은 일반적으로 남성보다 혈중 면역글로불린 M (immunoglobulin [Ig] M) 농도는 높지만 IgA 수치는 낮은 특성을 보이는데, 이는
C. difficile에 대한 점막 방어력을 저하시킬 수 있고 여성에서 관찰되는 높은 발생률이나 재발률의 원인이 될 수 있다[
101,
102]. 앞서 언급한 성별 차이를 고려할 때 프로바이오틱스 효능도 성별에 따라 다를 가능성이 있지만, 현재까지 성별 특이적 효능에 관한 근거는 불명확하다. 따라서 향후 프로바이오틱스 임상시험은 이러한 생물학적 차이를 반영해 세심하게 설계되어야 하며, 이는 궁극적으로 예방전략을 정교화하고 CDI 치료에 보다 개인 맞춤형 접근을 가능하게 할 것이다.
고찰
호르몬 차이, 마이크로바이옴 변이 및 치료반응
장내미생물은 IBS, IBD, 대장암 등 다양한 위장관질환에 기여하는 것으로 알려져 있다. 정확한 병인은 아직 불분명하나, 장내미생물이 장 운동성, 염증 및 면역반응에 미치는 영향에 대한 증거가 점차 증가하고 있다[
6,
103]. 최근에는 위장관질환에서 성별 차이와 장내미생물과의 관련성이 제시되고 있다[
5,
6,
103,
104]. 또한 에스트로젠과 안드로젠의 대사가 장내미생물과 밀접한 관련이 있음이 보고되었다. 장내미생물이 성호르몬의 분비 및 순환과정에 관여함이 알려지면서, 성호르몬이 장내미생물에 미치는 역할을 나타내는 “마이크로젠더로옴(microgenderome)” 개념이 제안된 바 있다. 에스트로젠과 테스토스테론은 장내미생물과 면역세포에 직접적인 영향을 미치는 것으로 나타났다. β-estradiol(에스트라다이올)은 수지상 세포의 형질 전환을 유도하여 interleukin (IL)-12 및 interferon-γ 생성을 촉진하며[
105], 이는 다시 염증성 사이토카인 경로를 활성화한다. 에스트라다이올은 B세포의 생존을 연장하고 다클론성 B세포를 활성화한다[
105]. 이렇게 조성된 염증성 환경과 변화된 장 투과성은 장내미생물이 고유판(lamina propria)으로 이동하는 원인이 되며, 이는 다시 염증과정을 촉진한다[
105]. 남성에서는 테스토스테론이 T 세포 증식을 억제하는 효과를 보이며 에스트라다이올과 달리 장벽기능을 변화시키지 않는다[
105]. 장내미생물은 뇌-장 축과 장벽기능 조절에 핵심적인 역할을 한다[
106-
108]. 단쇄지방산은 풍부하고 가장 중요한 미생물 대사 산물로, 장 운동성과 상처 치유를 조절하는 염증 조절자이다[
109]. 또한 미생물-장-뇌축 사이를 잇는 매개체로 밝혀졌다[
110-
112]. 흥미롭게도 부티르산 생성 장내미생물의 성별 차이가 보고된 바 있다[
100]. 추가적으로, 최근 연구에 따르면 oligofructose가 포함된 식단을 투여했을 때 암컷과 수컷 쥐의 장내미생물에서 서로 다른 단쇄지방산 프로파일이 나타났다. 암컷의 경우 oligofructose 보충이 Bacteroidetes의 풍부도를 증가시켰으나, 수컷에서는 차이가 없었다. 나아가 분변 내 낙산, 간 IgA, IL-6 및 맹장 IL-6 수치는 수컷에서 증가한 반면, IL-10 수치는 암컷에서 더 높았다[
113]. 흥미롭게도 토착 아프리카인들은
Faecalibacterium prausnitzii,
Clostridium cluster IV,
Clostridium cluster XIVa와 같은 부티르산 생성 박테리아가 현저히 풍부했으나, 아프리카계 미국인에서는
Bacteroides가 우세했다[
114]. 또한 성별 차이를 분석해보면
Bacteroides-
Prevotella 그룹은 남성에서 여성보다 더 높게 나타났다[
115]. 성별에 따른 프로바이오틱스 치료반응의 측면에서는, 루푸스 모델 쥐에 5종
Lactobacillus 균주 혼합물을 투여했을 때 여성과 거세된 수컷에서는 신장 기능이 개선되고 항염증 효과가 나타났으나, 생식기가 온전한 수컷에서는 효과가 없었다[
116]. 이는 프로바이오틱스 투여에 있어 성별 차이를 시사하지만, 대부분의 연구는 동물에서 수행되었다.
프로바이오틱스의 생물학적 효과는 균주의 특성과 숙주요인에 의해 영향을 받는데, 여기에는 생리, 면역 및 미생물 구성의 성별 차이 등이 포함된다. IBS와 같이 명확한 성차가 있는 질환에서는 치료반응도 성별에 따라 다를 가능성이 있다[
117]. 그러나 임상적 증거는 연구설계의 이질성과 성별 분석 부족으로 인해 아직 결론적이지 않다. 반면, 통제된 동물모델에서는 프로바이오틱스에 대한 성별 의존적 반응이 뚜렷하게 나타났으나, 이를 평가하기 위해 특별히 설계된 전임상 연구의 수는 여전히 부족한 실정이다(
Table 3).
반복적 물회피 스트레스(repeated water avoidance stress, rWAS) 모델과 같은 스트레스 유발 위장관질환 모델에서, 암컷 설치류는 수컷에 비해 전형적으로 심한 내장과민성, 비만세포 침윤, 과도한 점막 사이토카인 발현을 특징으로 하는 높은 취약성을 나타낸다. rWAS 모델연구에서
Companilactobacillus farciminis(구
Lactobacillus farciminis) 또는
Bifidobacterium longum BBH016을 10일간 경구 투여하면 암컷 쥐에서만 내장과민성과 대장 미세염증이 유의하게 감소했다[
118,
119]. 반면,
Roseburia faecis BBH024와 R22-12-24는 수컷 쥐에서 더 뚜렷한 항염증 효과를 나타내며 배변량을 줄이고 기능적 미생물 경로를 개선했다[
120]. 이와 유사한 성별 의존적 반응이 IBS 모델을 넘어 대사 및 면역 맥락에서도 관찰된다. 고지방 식이를 한 쥐에서
Clostridium butyricum IDCC 1301 투여에 의한 장 염증 완화 및 장벽 기능 개선효과는 성별에 따라 다르게 나타났다. 항염증 및 장벽 보호효과는 수컷에서 더 뚜렷한 반면, 암컷은 담즙산 프로필과 염증지표에서 독특한 변화를 보였다[
121]. 또한
C. butyricum IDCC 1301은 성별에 따라 장내미생물군을 다르게 재구성하여, 수컷에서 주로 부티르산 생성 균주를 증가시키고 암컷에서는
Akkermansia muciniphila를 더 현저히 감소시켰다[
122]. 이러한 결과는 스트레스로 유발된 장 기능장애가 성별 특이적 염증 및 미생물 반응을 유발하며, 이러한 반응들이 프로바이오틱스 균주뿐만 아니라 숙주의 성별에 따라서 다르게 조절된다는 점을 시사한다.
면역 및 신경행동 동물모델을 이용한 다른 연구들에서도 이와 유사한 성별 의존적 차이가 보고되었다.
Limosilactobacillus reuteri(구
Lactobacillus reuteri) DSMZ 8533 투여는 수컷과 암컷 사이에 뚜렷하게 다른 미생물 구성과 사이토카인의 변화를 일으켰다[
123]. 또한 태아기에 아편에 노출된 쥐에서 VSL#3 치료는 성별에 따라 장내미생물 불균형과 통각 변화가 다르게 개선되었는데, 수컷에서는 통증 민감도가 완화되었고 암컷에서는 미생물 프로필이 정상화되었다[
124]. 종합하면, 이러한 결과들은 성별 특이적인 프로바이오틱스 효과가 스트레스, 대사 및 통증을 조절하는 미생물 및 신경 면역축에 영향을 미친다는 점을 부각한다. 축적된 전임상 증거들은 프로바이오틱스의 효과가 성별에 따라 다르다는 점을 시사하며, 이는 호르몬 환경, 면역 활성화, 그리고 기초 장내미생물 무리의 차이에서 기인할 가능성이 높다. 이러한 실험적 결과들은 맞춤형 미생물 기반 치료로 발전시키기 위해 성별을 핵심적인 생물학적 변수로 고려해야 할 필요성을 강조한다.
검토한 임상 증거에 따르면, 프로바이오틱스는 하부 위장관질환 관리에 있어 미미하지만 유의한 잠재력을 보인다. IBS 환자에서는 특정 균주가 전반적인 증상, 특히 복통과 복부 팽만감을 완화할 수 있음을 시사하고 있다. FC에서는 일부 프로바이오틱스 및 신바이오틱스가 배변 횟수와 굳기를 개선한다. CDI에서는 1차 예방을 위한 일상적 사용은 여전히 논란의 여지가 있으나, 특정 고위험군에서 이점이 있을 수 있다. 그러나 연구 설계, 균주, 용량, 치료기간의 현저한 이질성으로 인해 이러한 결과를 임상에 적용하는 것은 여전히 어려움이 있다. 또한 대부분의 임상시험에서 서로 다른 제형을 사용하고 있어 균주 특이적 효과를 명확히 파악하기 어렵게 만들며, 표준화된 가이드라인의 수립을 복잡하게 한다. 특히 성별 차이에 관련하여 전임상 결과와 임상시험 사이의 불일치가 두드러진다. 통제된 실험환경의 동물모델에서는 특정 프로바이오틱스에 대해 뚜렷하고 강력한 성별 의존적 반응이 확인된 반면, 인간을 대상으로 한 임상시험에서는 아직 이러한 명확한 차이가 확인되지 않았다. 임상현장에서 유의미한 성별 특이적 근거가 부족한 이유는 대개 통계적 검정력의 부족한 연구 규모, 사후 분석, 또는 남성이나 여성 집단의 과소 대표성에서 기인한다. 따라서 현재로서는 환자의 성별에 근거하여 특정 프로바이오틱스 균주를 선택하도록 결정적인 임상 권고안을 제시하기는 어렵다. 그 대신, 향후 연구와 RCT에서는 이러한 성별 요소를 핵심적인 생물학적 변수로 우선적으로 고려해야 한다. 이처럼 명확한 근거가 부족한 현재 상황에서 임상의는 주요 증상과 근본적인 병태생리에 기반하여 균주를 선택하는 개인별 맞춤형 접근방식을 취해야 한다. 결과적으로, 임상의는 개별 환자의 다양성에도 불구하고 표준화되고 안전한 중재를 보장하기 위해 품질, 안정성, 환자별 위험요인을 포함한 프로바이오틱스의 실제적 이용과 안전성 측면에 대해 기본적인 이해를 갖추어야 한다.
임상의가 프로바이오틱스를 사용할 때 고려해야 할 사항은 무엇인가?
임상현장에서 프로바이오틱스의 사용이 크게 증가했음에도 불구하고, 제품의 다양성, 불명확한 라벨 표기, 표준화된 처방 가이드라인의 부재로 인해 임상의들은 여전히 어려움에 직면해 있다. 아래에서는 용량, 안정성, 제형 및 환자별 요인을 포함하여 임상의가 프로바이오틱스를 처방할 때 고려해야 할 요소들을 논의하고자 한다.
용량 및 제형에 따른 적응증
의사는 제조사의 문서를 통해 프로바이오틱스의 유통기간 동안 안정성과 생균 수(CFU) 유지 여부를 확인해야 한다. 임상적 이익을 얻기 위해서는 일반적으로 최소 1.0×10
9 CFU/일 투여량이 요구되나[
125-
127], 규제기준은 국가별로 다르다(한국: 1.0×10
8 CFU; EU/캐나다: 1.0×10
9 CFU 이상; 미국: 1.0×10
8–10
11 CFU/일)[
128,
129]. 고용량이 반드시 효능 향상으로 이어지는 것은 아니므로, 복용량은 임상시험을 통해 입증된 균주별 근거 용량을 따라야 한다[
130]. 제조사는 유통기한까지 생존 균수를 보장하기 위해, 제품에 표시된 용량보다 더 많은 양을 투여하여 제조(overage)하는 경우가 많다[
131]. 제형 측면에서는 일반적으로 액상 현탁액보다 캡슐이나 분말과 같은 고형 제제가 더 높은 안정성을 보인다[
132]. 최근에는 마이크로캡슐화 및 나노기술과 같은 진보된 기술이 도입되어 특정 부위로의 전달 효율을 최적화하고 있다[
133].
프로바이오틱스 복용 시점
프로바이오틱스의 생존과 정착은 식사시간, 생체리듬, 그리고 병용 약물의 영향을 받는다. 공복상태의 위내 강산성 환경은 세균의 생존율을 저하시키므로, 프로바이오틱스는 식사 중 또는 식사 직후에 복용하는 것이 통과 생존율을 높이며, 특히 지방이 포함된 식단과 함께 섭취할 때 더욱 효과적이다[
134]. 동물실험에서는 숙주-미생물 상호작용에 일주기(diurnal) 변동이 관찰되지만, 인간에서는 특정 시간대에 복용을 권고할 충분한 증거는 없다[
135]. IBS, 감염성 설사, IBD 등에 관한 메타분석에서는 정확한 복용시간보다 매일 꾸준한 복용이 더 중요하다고 제시하고 있다[
2,
136]. 아침이나 저녁 등 복용 시간대와 상관없이, 복약순응도가 프로바이오틱스 효능의 강력한 예측인자로 작용한다. 항생제와 병용할 경우 직접적 비활성화를 방지하기 위해 2–3시간 간격을 두는 것이 권장된다.
프로바이오틱스 효능에 영향을 미치는 숙주 요인
프로바이오틱스 효과는 여러 주요 요인의 개인 간 변이성에 결정적인 영향을 받는다. 각 개인의 장내미생물은 기저 다양성과 정착 저항성이 프로바이오틱스의 성공적인 정착을 결정하는 일차적 요인이므로 핵심적인 역할을 한다[
137]. 선천면역 수용체(예: Toll-like receptors 또는 nucleotide-binding oligomerization-containing domain 2)의 유전자 다형성은 숙주와 미생물 간 상호작용에 영향을 미쳐 점막 면역을 조절하는 프로바이오틱스의 효능을 변화시킬 수 있다[
138]. 연령도 효능에 영향을 미치며, 영유아의 미성숙 면역계와 노인의 노화된 면역계는 정착 잠재력을 다르게 나타낸다[
139,
140]. 또한 식습관은 생존 및 지속성에 영향을 미치는데, 지방은 위 통과 시 프로바이오틱스 생존력을 높이고 섬유질은 프리바이오틱 기질로 작용한다[
141]. 마지막으로, 환자의 면역상태나 양성자펌프억제제(proton pump inhibitor), 면역억제제 등의 현재 복용 중인 약물도 투여된 프로바이오틱스의 생존 및 기능적 반응을 변화시킬 수 있다[
142,
143].
프로바이오틱스 안전성
프로바이오틱스는 일반적으로 안전성이 우수하며, 가장 흔한 부작용은 경미한 위장관 증상(복부팽만, 가스)이다[
144,
145]. 그러나 안전성 데이터는 사용된 균주와 제형에 따라 크게 다르며, 대부분의 임상시험은 부작용 보고의 미비나 장기적 위험평가를 위한 추적관찰 부족 등 방법론적 한계를 지니고 있다[
146]. 실제 임상 데이터(Food and Drug Administration Adverse Event Reporting System 2005–2023)에서는 심각한 부작용 발생률이 매우 낮게 보고된다[
147]. 그러나 성별에 따른 차이, 불명확한 제품 표기, 그리고 보고된 부작용 사례 자체가 적다는 점 때문에 이러한 결과가 실제 생물학적 차이를 온전히 반영하지 못할 가능성이 있다. 따라서 결과 해석에 주의가 필요하며, 향후 연구에서는 성별 층화 분석, 충분한 표본 크기 및 장기적인 모니터링을 반드시 갖추어야 한다. 중환자실 환자, 중심정맥관 보유자, 심한 면역억제 환자 등 고위험군에서는 미생물 전이(translocation)로 인한 균혈증이나 진균혈증 등의 드문 위험성이 보고되고 있다[
148-
150]. PROPATRIA 연구에서 사망률 증가 원인은 프로바이오틱스 병원성보다는 특정 대사인자로 밝혀졌다[
148]. 또한 제조 및 유통과정에서 오염 또는 라벨링 오류로 인해 의도하지 않은 병원성 미생물에 노출될 수 있다[
144,
146,
151,
152]. 따라서 프로바이오틱스 사용 시 안전성과 연관된 다양한 측면을 고려해야 하고, 임상에서는 프로바이오틱스 사용 후 부작용 신호를 인지하는 것이 필수적이다[
144,
146,
151,
152]. 다만, 위에서 언급한 위험들은 매우 드물며, 특정 조건 아래에서만 발생함을 강조할 필요가 있다[
153].
균주 특이적이며 충분한 검정력을 갖춘 RCT의 필요성
프로바이오틱스가 마치 하나의 균질한 치료군인 것처럼 논의되기도 하지만, 축적된 증거들은 이들의 임상적 효과가 매우 균주 특이적(strain-specific)임을 명확히 보여준다. IBS와 FC에서 대부분의 RCT는 작용기전, 용량, 생존력 특성이 서로 다른 여러 균주를 이용해 만들어진 다양한 제형의 프로바이오틱스 제품을 평가해왔다. 이러한 이질성은 결과를 해석하거나 재현하기 매우 어려우며, 성별에 따른 효능 평가와 같은 정밀한 하위 그룹 분석을 어렵게 만든다. 또한 많은 연구가 임상적으로 의미 있는 효과를 감지하기에 통계적 검정력이 부족하며, 특히 성별로 층화할 경우 더욱 그렇다. 프로바이오틱스에 대한 반응이 질환의 표현형뿐 아니라 복용자의 성별에 따라 다를 수 있으므로, 향후 RCT는 균주 특이적 분석과 성별 기반 분석이 가능하도록 충분한 표본 크기를 확보하여 설계되어야 한다.
표준화되고 임상적으로 유의미한 평가지표의 필요성
현재까지 축적된 근거들이 가진 또 다른 주요 한계는 표준화된 임상 평가지표의 부재이다. IBS, FC, CDI에서 프로바이오틱스를 평가한 연구들은 전반적 증상 개선, 개별 증상 점수, 배변 빈도, 대변 굳기, 삶의 질, 다양한 복합 평가지표 등 매우 광범위한 결과지표를 사용했다. 이러한 지표의 다양성은 메타분석 시 결과의 불균질성을 높이는 원인이 되며, 연구 간 비교를 어렵게 만든다. 향후 연구에서는 서로 조율되고 검증된 결과지표를 도입해야 한다.
임상연구 내 남녀 참여 불균형 및 대표성 부족
IBS, FC, CDI의 유병률과 병태생리, 그리고 임상적 양상에서 성별 차이가 이미 잘 알려졌음에도 불구하고, 대부분의 프로바이오틱스 연구는 성별을 생물학적 변수로 고려하지 않고 설계되었다. 많은 연구가 정당한 근거 없이 남성이나 여성 중 어느 한쪽 성별에 치우친 집단을 대상으로 진행되었다. 또한 일부 임상시험에서는 성별 분석이 탐색적이거나 사후 분석에 그쳐 그 결과를 타당하게 해석하는 데 한계가 있다. 이러한 불균형은 통계적 검정력을 저하시킬 뿐 아니라 효능 및 안전성 측면에서 임상적으로 유의미한 차이를 가릴 위험이 있다. 개인 맞춤형 프로바이오틱스 치료로 나아가기 위해서는, 향후 임상시험에서 남녀 피험자를 균형 있게 모집하고, 성별 기반 하위 그룹 분석을 사전에 계획하며, 성별로 세분화된 결과를 투명하게 보고해야 한다.
성별 기반 가설의 기전적 검증 필요성
전임상 연구는 프로바이오틱스가 장 염증, 내장감각, 면역반응, 미생물 구성에 대해 남녀 간 현저히 다른 영향을 미칠 수 있다는 강력한 증거를 제시해왔다. 이는 성별에 따라 프로바이오틱스의 효능이 달라질 수 있다는 생물학적 타당성을 뒷받침한다. 그러나 인간 연구에서의 기전적 검증은 여전히 제한적이다. 대부분의 임상시험은 미생물의 기능적 프로파일, 면역지표, 상피 장벽 마커, 또는 호르몬과 장내미생물 무리의 상호작용과 같은 기전적 바이오마커를 통합하지 않은 채, 증상 기반의 결과에만 의존하고 있다. 향후 연구는 잘 설계된 임상시험에 이러한 기전적 평가지표를 포함함으로써, 기초연구와 임상시험 사이의 연구 간 간극을 메워야 한다.
결론
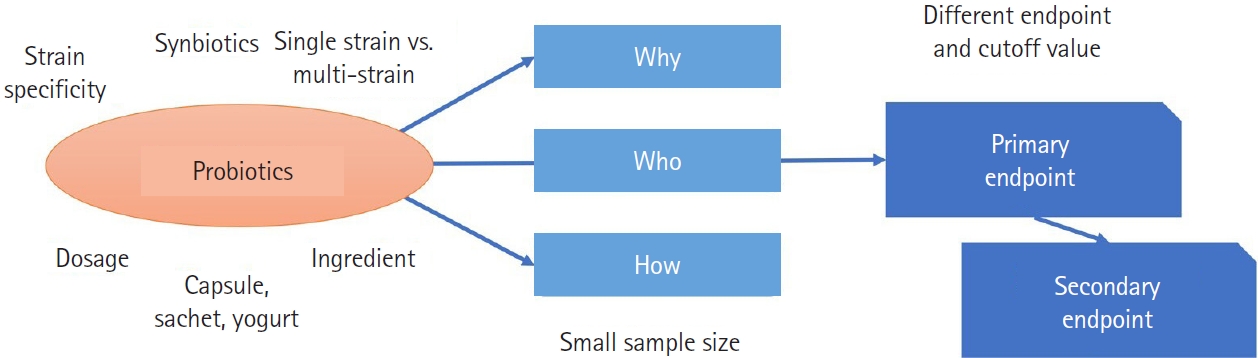
프로바이오틱스를 이용한 IBS, FC, CDI 치료에 있어 현재 이용 가능한 데이터들은 균주, 용량, 그리고 연구설계의 다양성으로 인해 여전히 일관성이 부족하다(
Fig. 4). 그러나 일부 환자에서 배변 습관과 증상 정도가 개선되었고, 동물실험에서는 성별 차이가 있다는 명확한 증거가 제시되었다. 특히 IBS와 FC가 여성에게서 뚜렷하게 많이 나타난다는 점을 고려할 때, 성별과 관련된 생물학적 기전에 대한 심도 있는 고려가 필요하다. 성별에 따른 프로바이오틱스의 기전적ㆍ임상적 효과를 규명하기 위해 대대적인 체계적 노력이 요구되며, 이러한 노력은 결국 환자 개개인에게 최적화된 맞춤형 프로바이오틱스 전략을 수립하는 데 크게 기여할 것이다.
-
Authors’ contribution
Conceptualization: YSK, NK, MIP. Project administration: NK, MIP. Methodology: NK. Investigation (literature review): YSK, SYP, SJK, MWL, YC, BYK, CMS, YSnK (Young Sun Kim). Data curation: SYP, SJK. Visualization (tables): SYP, SJK. Supervision: NK, MIP. Funding acquisition: NK. Writing–original draft: YSK (lead), SYP, SJK, MWL, YC, BYK, CMS, YSnK, NK. Writing–review and editing: YSK, SYP, SJK, MWL, YC, BYK, CMS, YSnK, MC, NK, MIP.
-
Conflict of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This research was supported by the National Institute of Health (NIH) research project (Project No. 2025-ER1104-00).
-
Data availability
Not applicable.
-
Acknowledgments
None.
Supplementary materials
Fig. 1.Meta-analysis of studies reporting sex differences in the efficacy of probiotics in irritable bowel syndrome. (A) Total population. (B) According to sex (in probiotics group). CI, confidence interval; M-H, Mantel-Haenszel; df, degrees of freedom.
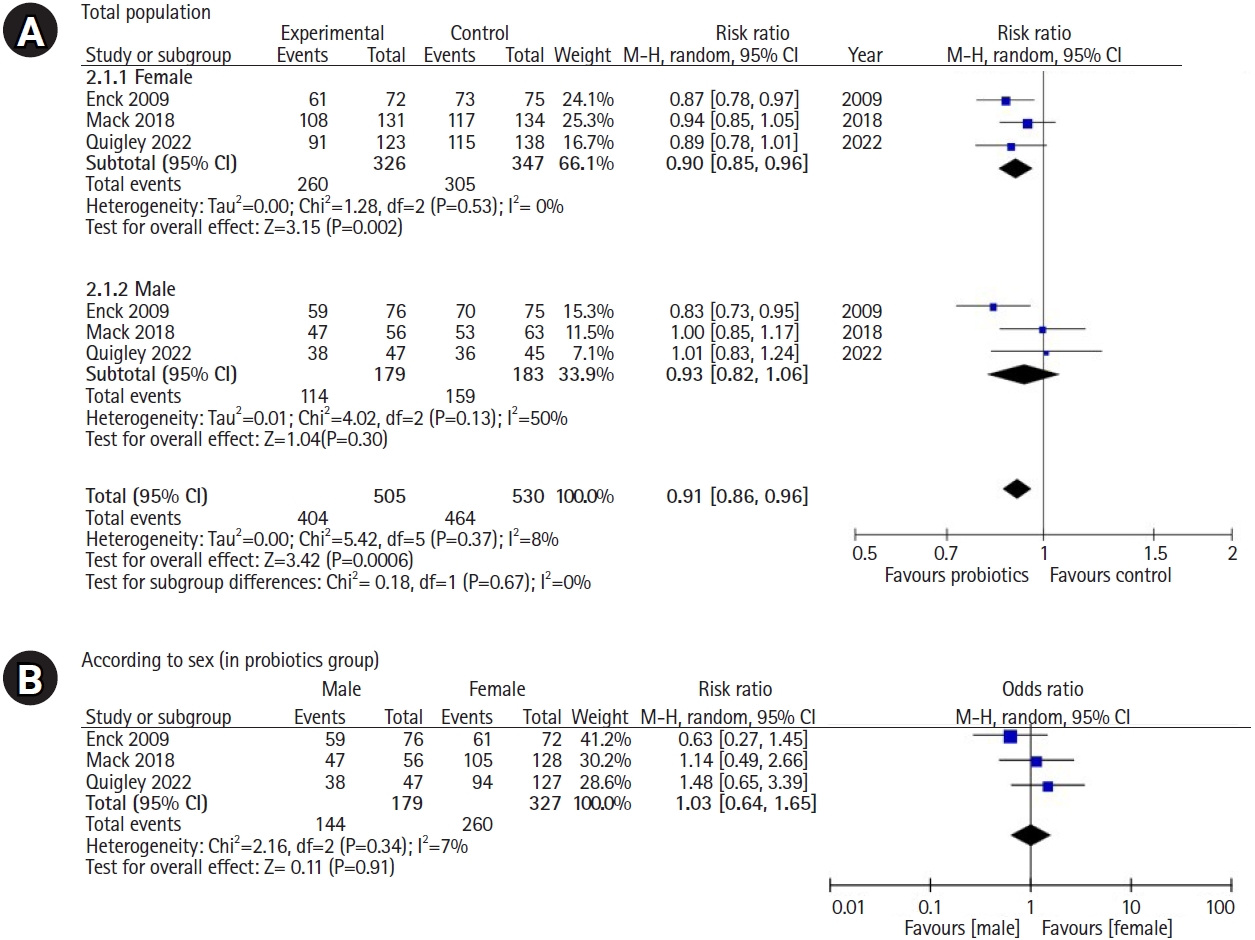
Fig. 2.Change of spontaneous bowel movement by species. SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom.
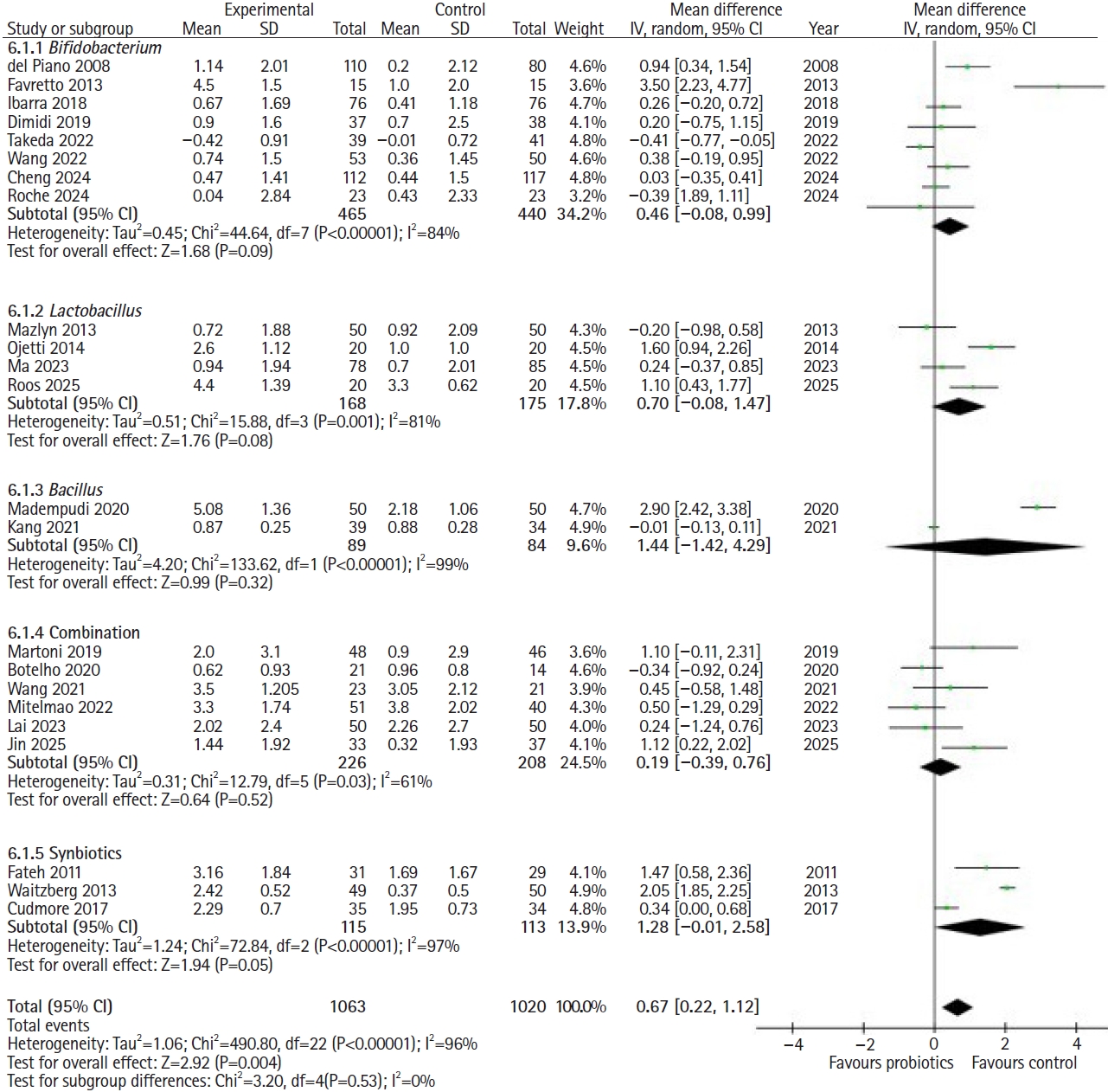
Fig. 3.Change of stool consistency (Bristol stool form scale) by species. SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom.
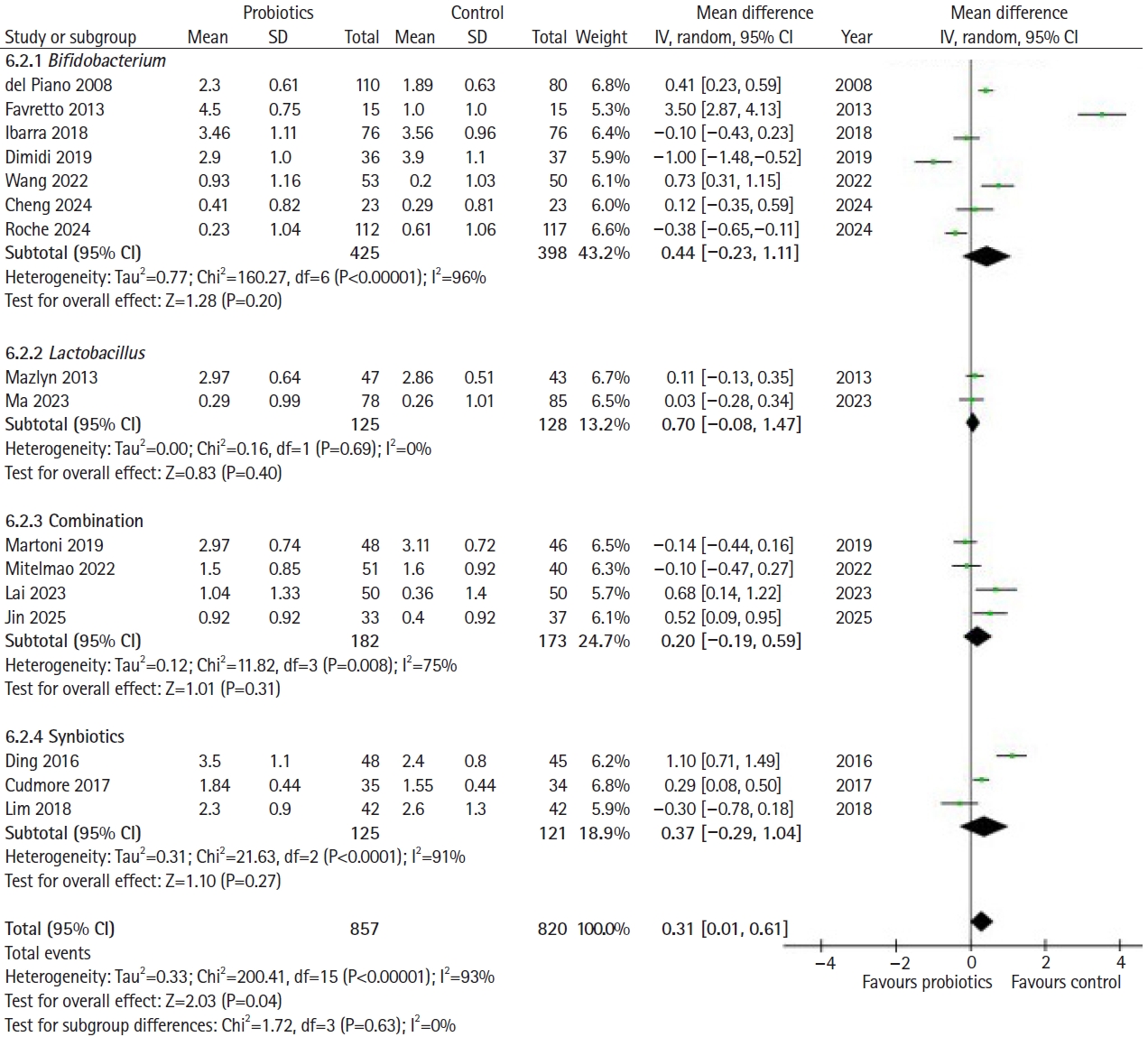
Fig. 4.Factors contributing to heterogeneity in probiotic clinical trials.
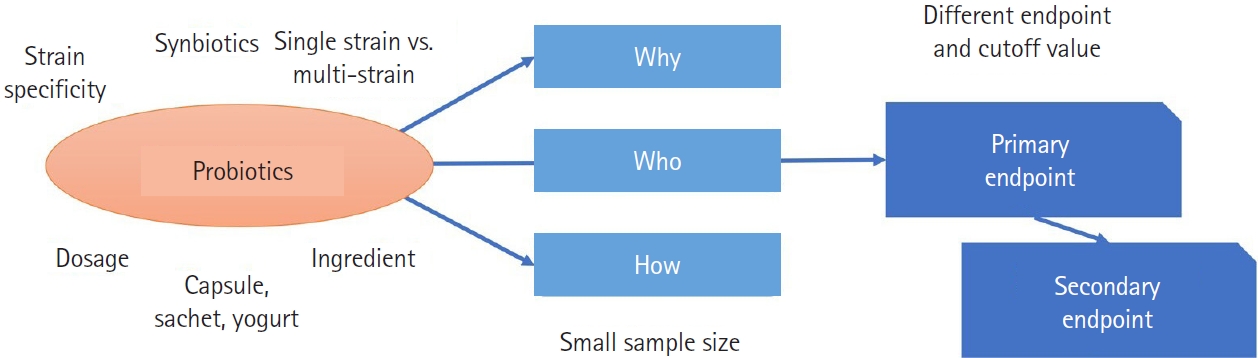
Table 1.Studies reporting sex differences in the efficacy of probiotics in irritable bowel syndrome
|
Study (year) |
Country |
Patients |
Probioticsa)
|
CFU |
Total |
Treatment group |
Control group |
Duration (wk) |
Primary outcome |
Results |
|
Male |
Female |
Male |
Female |
Male |
Female |
|
Enck [31] (2008) |
Germany |
NA |
E. coli DSM 17252, E. faecalis DSM 16440 |
1.35×108–4.05×108
|
150 |
147 |
77 |
72 |
73 |
75 |
8 |
Global symptoms and abdominal pain |
NNT: males 2.49 (1.76–4.22), females 3.98 (2.55–9.13) |
|
Enck [32] (2009) |
Germany |
NA |
E. coli DSM 17252 |
6.8×107–2.0×108
|
151 |
147 |
76 |
72 |
75 |
75 |
8 |
Global symptoms and abdominal pain |
Responder rate: males 22.6% vs. 7.2%, females 15.5% vs. 2.5% |
|
Ludidi [33] (2014) |
The Netherlands |
Rome III |
L. casei W56, L. salivarius W57, L. lactis W58, L. acidophilus NCFM, L. rhamnosus W71 |
5.0×109
|
13 |
27 |
6 |
15 |
7 |
12 |
6 |
Abdominal pain (visceral perception) |
MSS: males −1.18 (−1.80 to −0.25) vs. 0.93 (−3.87 to 1.43), females −0.06 (−3.77 to 1.64) vs. −1.49 (−7.42 to −0.32) |
|
Mack [34] (2022) |
Germany |
Rome III |
E. coli DSM 17252, E. faecalis DSM 16440 |
1.3×10⁸–3.9×10⁸ |
187 |
197 |
56 |
131 |
63 |
134 |
26 |
Global symptoms and abdominal pain |
IBS-GAI: males 16.1% vs. 17.2%, females 18.0% vs. 13.1% |
|
Quigley [35] (2023) |
USA, UK/Ireland |
Rome IV |
B. hydrogenotrophica
|
2.0×1010–2.0×1011
|
96 |
269 |
50 |
127 |
46 |
142 |
8 |
Bowel habit and abdominal pain |
Overall response: males 19.1% vs. 20.0%, females 26.0% vs. 16.7% |
|
Preston [36] (2018) |
US, Canada |
Rome III |
L. acidophilus CL1285, L. casei LBC80R, L. rhamnosus CLR2 |
1.0×1011
|
45 |
68 |
16 |
21 |
29 |
47 |
12 |
Global symptoms and abdominal pain |
Improvement in QOL; IBS-D only in males |
|
Chang [37] (2024) |
South Korea |
Rome III |
B. longum IDCC 4101, B. bifidum IDCC 4201, B. lactis IDCC 4301, B. breve IDCC 4401, E. faecium IDCC 2102, L. rhamnosus IDCC 3201, L. acidophilus IDCC 3302, L. casei IDCC 3451, L. plantarum IDCC 3501, L. helveticus IDCC 3801 |
1.0×1010
|
39 |
53 |
26 |
21 |
13 |
32 |
4 |
Global symptoms |
Overall IBS symptom relief: males 3.54±0.42 vs. 2.69±0.44, females 3.48±0.32 vs. 2.40±0.28 |
Table 2.Characteristics of studies using probiotics in patients with constipation
|
Year |
Country |
Patients |
Probioticsa)
|
CFU |
Treatment group:control group |
Duration |
Outcome |
|
del Piano [50] (2008) |
Italy |
Evacuation disorder |
L. plantarum, B. animalis lactis
|
5.0×109
|
80:110:110b)
|
30 days |
Increase in number of weekly evacuations in probiotics group |
|
Fateh [51] (2011) |
Iran |
FC (Rome III) |
B. longum, B. breve, L. casei, L. rhamnosus, S. thermophilus, FOS |
1.0×108
|
31:29 |
4 wk |
Increase in stool frequency in men receiving probiotics |
|
Favretto [52] (2013) |
Brazil |
FC (Rome III) |
B. lactis Bi-07 |
1.0×108
|
15:15 |
30 days |
Increase in stool frequency in women receiving probiotics |
|
Mazlyn [53] (2013) |
Malaysia |
FC (Rome III) |
L. casei Shirota |
3.0×1010
|
50:50 |
4 wk |
Probiotics did not alleviate constipation severity, stool frequency, and consistency. |
|
Waitzberg [54] (2013) |
Brazil |
FC (Rome III) |
B. lactis, L. paracasei, L. rhamnosus, L. acidophilus, and FOS |
<109
|
49:50 |
30 days |
Synbiotics improved stool frequency and consistency in constipated women. |
|
Ojetti [55] (2014) |
Italy |
FC (Rome III) |
L. reuteri DSM17938 |
1.0×108
|
20:20 |
4 wk |
Probiotics increased stool frequency. No difference in stool consistency. |
|
Ding [56] (2016) |
China |
FC (Rome III) |
B. longum, L. acidophilus, E. faecalis, soluble fiber (Pectin) |
3.0×107
|
48:45 |
12 wk |
Synbiotic exhibited increased stool; Frequency and improved stool consistency and constipation-related symptoms. |
|
Cudmore [57] (2017) |
Ireland |
FC (Rome III) |
B. bifidum, L. rhamnosus, L. acidophilus, psyllium/inulin |
6.0×108
|
35:34 |
4 wk |
Synbiotics did not significantly improve stool frequency. |
|
Ibarra [58] (2018) |
France |
FC (Rome III) |
B. animalis HN019 |
1.0×109/1010
|
76:76:76c)
|
4 wk |
No difference in stool frequency and consistency between the probiotics and placebo groups. |
|
Lim [59] (2018) |
Malaysia |
FC (Rome III) |
B. lactis BB12, L. plantarum LP01, inulin-oligofructose |
1.0×1010
|
43:42 |
12 wk |
No difference in stool frequency and consistency between the probiotics and placebo groups. |
|
Dimidi [60] (2019) |
UK |
FC (Rome III) |
B. lactis
|
1.5×1010
|
37:38 |
4 wk |
There were also no improvements in stool output, symptoms, or quality of life between probiotics and placebo groups. |
|
Martoni [61] (2019) |
Canada |
FC (Rome III) |
L. acidophilus, B. animalis lactis, B. longum, B. bifidum
|
1.5×1010
|
48:46 |
4 wk |
No difference in stool frequency and consistency between the probiotics and placebo groups. |
|
Botelho [62] (2020) |
Brazil |
FC (Rome IV) |
L. acidophilus, L. casei, L. lactis, B. bifidum, B. lactis
|
5.0×109
|
21:14 |
30 days |
Probiotics improved constipation-related symptoms. |
|
Madempudi [63] (2020) |
India |
FC (Rome III) |
B. coagulans Unique IS2 |
2.0×1010
|
50:50 |
4 wk |
Probiotics improved stool frequency and consistency. |
|
Kang [64] (2021) |
South Korea |
FC (Rome III) |
B. coagulans SNZ1969 |
1.0×109
|
40:40 |
8 wk |
Probiotics improved stool frequency and colon transit time. |
|
Wang [65] (2021) |
China |
FC (Rome III) |
S. thermophilus, L. bulgaricus, B. animalis
|
1.0×1010
|
23:21 |
4 wk |
Probiotics improved constipation-related symptoms. |
|
Mitelmao [66] (2022) |
Brazil |
FC (Rome IV) |
Multiple combination of Lactobacillus and Bifidobacterium
|
8.0×109
|
51:51 |
30 days |
Probiotics improved stool frequency and consistency. |
|
Takeda [67] (2022) |
Japan |
FC (Rome IV) and elderly (>65) |
B. longum BB536 |
5.0×1010
|
39:41 |
4 wk |
Probiotics improved stool frequency in elderly patients. |
|
Wang [68] (2022) |
China |
FC (Rome IV) |
B. bifidum CCFM16 |
2.0×109
|
53:50 |
4 wk |
Probiotics improved stool consistency. |
|
Lai [69] (2023) |
China |
FC (Rome IV) |
B. animalis subsp. lactis HN019, L. rhamnosus HN0001 |
|
50:50 |
4 wk |
Probiotics improved stool consistency and constipation-related symptoms, but did not increase stool frequency. |
|
Ma [70] (2023) |
China |
FC (Rome IV) |
L. plantarum P9 |
1.0×1011
|
78:85 |
4 wk, 6 wk |
Probiotics significantly improved stool frequency and symptoms. |
|
Cheng [71] (2024) |
China |
FC (Rome IV) |
B. animalis subsp. lactis HN019 |
7.0×109
|
112:117 |
8 wk |
No difference in stool frequency in probiotics and placebo groups. |
|
Salo [72] (2024) |
Spain |
Constipation |
B. animalis subsp. lactis BLa80 |
2.0×109
|
23:23 |
4 wk, 8 wk |
Probiotics improved stool frequency. |
|
Jin [73] (2025) |
South Korea |
Constipation |
Multiple combination of Lactobacillus and Bifidobacterium
|
2.0×109
|
33:37 |
4 wk, 8 wk |
Probiotics significantly improved stool frequency, consistency and symptoms. |
|
Roos [74] (2025) |
Sweden |
Constipation |
L. gasseri
|
1.0×109
|
20:20 |
4 wk |
Probiotics improved constipation-related symptoms in women. |
Table 3.Summary of preclinical studies investigating sex-dependent effects of probiotics
|
Study (year) |
Animal, model |
Probiotics |
CFU/day/rat |
Experimental design |
Sex-dependent results |
|
Lee [118] (2017) |
Wistar rats; rWAS (1 hr/day for 10 days) |
C. farciminis
|
1.0×10¹¹; 10 days during rWAS |
3 groups (no-stress, rWAS, rWAS + C. farciminis) |
• Female: rWAS → ↑FPO, visceral analgesia, ↑mast cells & proinflammatory cytokines; Probiotics → ↓mast cells, ↓IFN-γ, ↓TNF-α, ↓IL-6, ↓PRSS1-3 |
|
• Male: rWAS → mild ↑FPO, no analgesia; Probiotics → no reduction in inflammation, ↑IL-1β, ↑IL-17 |
|
Choi [119] (2024) |
Wistar rats; rWAS (1 hr/day for 10 days) |
B. longum BBH016 |
1.0×109; 10 days during rWAS |
3 groups (control, rWAS, rWAS + B. longum) |
• Females: rWAS → ↑FPO, ↑mast cells, dysbiosis; Probiotics → ↓FPO, ↓mast cells, mitigated dysbiosis |
|
• Males: rWAS → ↑FPO; Probiotics → no significant effect |
|
Choi [120] (2023) |
Wistar rats; rWAS (1 hr/day×10 days) |
R. faecis BBH024 and R22-12-24 |
1.0×109; 10 days during rWAS |
3 groups (control, rWAS, WAS + R. faecis) |
• Female: rWAS → ↑FPO, ↑mast cells; probiotics → ↓FPO, ↑IL-6 |
|
• Male: rWAS → ↑FPO, ↑mast cells, ↑IL-6; Probiotics → ↓FPO, ↓mast cells, ↓IL-6 |
|
Choi [121] (2023) |
Fischer-344 rats, HFD (8 wk) |
C. butyricum IDCC 1301, Biovita |
Low 1×10⁷; Medium 1×10⁸; High 1×10⁹; 8 weeks during HFD |
5 groups (control, Biovita, C. butyricum at low/medium/high concentrations) |
• Female: HFD → ↓TJPs, ↑MPO, ↓butyrate, ↓IL-6; Probiotics → ↑TJPs, ↑IL-6 |
|
• Male: HFD → ↑TJPs, ↑TNF-α, ↑MPO, ↓butyrate; Probiotics → ↓TNF-α, ↓ MPO, ↑IL-10, ↑butyrate |
|
Choi [122] (2024) |
Fischer-344 rats, HFD (8 wk) |
C. butyricum IDCC 1301, Biovita |
Low 1×10⁷; Medium 1×10⁸; High 1×10⁹; 8 weeks during HFD |
5 groups (control, Biovita, C. butyricum at low/medium/high dose) |
• Female: HFD → ↓α-diversity, ↓Ruminococcaceae, ↑Lachnospiraceae, ↑A. muciniphila, altered carbohydrate/energy metabolism; Probiotics → ↑Ruminococcaceae, ↓A. muciniphila
|
|
• Male: HFD → ↓Ruminococcaceae, ↑A. muciniphila, ↓energy metabolism, altered carbohydrate/energy metabolism; Probiotics → ↑Lachnospiraceae, ↓A. muciniphila, recovered carbohydrate/energy metabolism |
|
He [123] (2019) |
BALB/c mice, healthy |
L. reuteri DSMZ 8533 |
Low 1.0×108; High 1.0×1010; 28 days |
3 groups (control, L. reuteri at low/high dose) |
• Females:, ↑ Helicobacter ↓Actinobacteria |
|
• Males: ↓ Bacteroides, ↓Prevotella, ↑ Clostridium IV |
|
Singh [124] (2025) |
C57BL/6 mice, POE |
VSL#3 |
4.5×1011; Late gestation–postnatal day 21 |
2 groups (POE only, POE + VSL#3) |
• Females: POE → ↓α-diversity, analgesia; Maternal probiotics → partial, transient normalization of analgesia |
|
• Males: POE → ↑α-diversity, hyperalgesia; Maternal probiotics → robust normalization of hyperalgesia |
References
- 1. Choi Y, Youn YH, Kang SJ, Shin JE, Cho YS, Jung YS, Shin SY, Huh CW, Lee YJ, Koo HS, Nam K, Lee HS, Kim DH, Park YH, Kim MC, Song HY, Yoon SH, Lee SY, Choi M, Park MI, Sung IK. 2025 Seoul Consensus on Clinical Practice Guidelines for Irritable Bowel Syndrome. J Neurogastroenterol Motil 2025;31:133-169. https://doi.org/10.5056/jnm25007
- 2. Ford AC, Quigley EM, Lacy BE, Lembo AJ, Saito YA, Schiller LR, Soffer EE, Spiegel BM, Moayyedi P. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: systematic review and meta-analysis. Am J Gastroenterol 2014;109:1547-1561. https://doi.org/10.1038/ajg.2014.202
- 3. Williams MD, Ha CY, Ciorba MA. Probiotics as therapy in gastroenterology: a study of physician opinions and recommendations. J Clin Gastroenterol 2010;44:631-636. https://doi.org/10.1097/MCG.0b013e3181d47f5b
- 4. Markle JG, Frank DN, Mortin-Toth S, Robertson CE, Feazel LM, Rolle-Kampczyk U, von Bergen M, McCoy KD, Macpherson AJ, Danska JS. Sex differences in the gut microbiome drive hormone-dependent regulation of autoimmunity. Science 2013;339:1084-1088. https://doi.org/10.1126/science.1233521
- 5. Kim N. Colorectal diseases and gut microbiome. In: Kim N, editor. Sex/gender-specific medicine in clinical areas. Springer; 2024. p. 137-208. https://doi.org/10.1007/978-981-97-0130-8_6
- 6. Kim YS, Unno T, Kim BY, Park MS. Sex differences in gut microbiota. World J Mens Health 2020;38:48-60. https://doi.org/10.5534/wjmh.190009
- 7. Goodoory VC, Khasawneh M, Black CJ, Quigley EMM, Moayyedi P, Ford AC. Efficacy of probiotics in irritable bowel syndrome: systematic review and meta-analysis. Gastroenterology 2023;165:1206-1218. https://doi.org/10.1053/j.gastro.2023.07.018
- 8. Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R. Bowel disorders. Gastroenterology 2016 Feb 18 [Epub]. https://doi.org/10.1053/j.gastro.2016.02.031
- 9. Lovell RM, Ford AC. Effect of gender on prevalence of irritable bowel syndrome in the community: systematic review and meta-analysis. Am J Gastroenterol 2012;107:991-1000. https://doi.org/10.1038/ajg.2012.131
- 10. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol 2012;10:712-721. https://doi.org/10.1016/j.cgh.2012.02.029
- 11. Holtmann GJ, Ford AC, Talley NJ. Pathophysiology of irritable bowel syndrome. Lancet Gastroenterol Hepatol 2016;1:133-146. https://doi.org/10.1016/S2468-1253(16)30023-1
- 12. Johanson JF, Kralstein J. Chronic constipation: a survey of the patient perspective. Aliment Pharmacol Ther 2007;25:599-608. https://doi.org/10.1111/j.1365-2036.2006.03238.x
- 13. Olafsdottir LB, Gudjonsson H, Jonsdottir HH, Jonsson JS, Bjornsson E, Thjodleifsson B. Irritable bowel syndrome: physicians’ awareness and patients’ experience. World J Gastroenterol 2012;18:3715-3720. https://doi.org/10.3748/wjg.v18.i28.3715
- 14. Kassinen A, Krogius-Kurikka L, Mäkivuokko H, Rinttilä T, Paulin L, Corander J, Malinen E, Apajalahti J, Palva A. The fecal microbiota of irritable bowel syndrome patients differs significantly from that of healthy subjects. Gastroenterology 2007;133:24-33. https://doi.org/10.1053/j.gastro.2007.04.005
- 15. Attaluri A, Jackson M, Valestin J, Rao SS. Methanogenic flora is associated with altered colonic transit but not stool characteristics in constipation without IBS. Am J Gastroenterol 2010;105:1407-1411. https://doi.org/10.1038/ajg.2009.655
- 16. Moayyedi P, Ford AC, Talley NJ, Cremonini F, Foxx-Orenstein AE, Brandt LJ, Quigley EM. The efficacy of probiotics in the treatment of irritable bowel syndrome: a systematic review. Gut 2010;59:325-332. https://doi.org/10.1136/gut.2008.167270
- 17. Vasant DH, Paine PA, Black CJ, Houghton LA, Everitt HA, Corsetti M, Agrawal A, Aziz I, Farmer AD, Eugenicos MP, Moss-Morris R, Yiannakou Y, Ford AC. British Society of Gastroenterology guidelines on the management of irritable bowel syndrome. Gut 2021;70:1214-1240. https://doi.org/10.1136/gutjnl-2021-324598
- 18. Lacy BE, Pimentel M, Brenner DM, Chey WD, Keefer LA, Long MD, Moshiree B. ACG Clinical Guideline: management of irritable bowel syndrome. Am J Gastroenterol 2021;116:17-44. https://doi.org/10.14309/ajg.0000000000001036
- 19. Dale HF, Rasmussen SH, Asiller ÖÖ, Lied GA. Probiotics in irritable bowel syndrome: an up-to-date systematic review. Nutrients 2019;11:2048. https://doi.org/10.3390/nu11092048
- 20. Cremon C, Guglielmetti S, Gargari G, Taverniti V, Castellazzi AM, Valsecchi C, Tagliacarne C, Fiore W, Bellini M, Bertani L, Gambaccini D, Cicala M, Germanà B, Vecchi M, Pagano I, Barbaro MR, Bellacosa L, Stanghellini V, Barbara G. Effect of Lactobacillus paracasei CNCM I-1572 on symptoms, gut microbiota, short chain fatty acids, and immune activation in patients with irritable bowel syndrome: a pilot randomized clinical trial. United European Gastroenterol J 2018;6:604-613. https://doi.org/10.1177/2050640617736478
- 21. Laterza L, Cremon C, Coppola G, Settanni CR, Maresca R, Strazzeri M, Durini E, Petito V, Scaldaferri F, Gargari G, Mora D, Vojoudi Yazdi E, Marangelo C, Ianiro G, Putignani L, Barbaro MR, Marasco G, Barbara G, Gasbarrini A. Multistrain probiotics plus vitamin D improve gut barrier function and gut microbiota composition in irritable bowel syndrome without constipation: results from a double-blind, randomized, placebo-controlled trial. Nutrients 2025;17:1708. https://doi.org/10.3390/nu17101708
- 22. Parkes GC, Sanderson JD, Whelan K. Treating irritable bowel syndrome with probiotics: the evidence. Proc Nutr Soc 2010;69:187-194. https://doi.org/10.1017/S002966511000011X
- 23. Nobaek S, Johansson ML, Molin G, Ahrné S, Jeppsson B. Alteration of intestinal microflora is associated with reduction in abdominal bloating and pain in patients with irritable bowel syndrome. Am J Gastroenterol 2000;95:1231-1238. https://doi.org/10.1111/j.1572-0241.2000.02015.x
- 24. Niedzielin K, Kordecki H, Birkenfeld B. A controlled, double-blind, randomized study on the efficacy of Lactobacillus plantarum 299V in patients with irritable bowel syndrome. Eur J Gastroenterol Hepatol 2001;13:1143-1147. https://doi.org/10.1097/00042737-200110000-00004
- 25. Simren M, Syrous A, Lindh A, Abrahamsson H. T2043 Effects of Lactobacillus plantarum 299v on symptoms and rectal sensitivity in patients with irritable bowel syndrome (IBS): a randomized, double-blind controlled trial. Gastroenterology 2006;130(4 suppl 2):A600.
- 26. Ducrotté P, Sawant P, Jayanthi V. Clinical trial: Lactobacillus plantarum 299v (DSM 9843) improves symptoms of irritable bowel syndrome. World J Gastroenterol 2012;18:4012-4018. https://doi.org/10.3748/wjg.v18.i30.4012
- 27. Stevenson C, Blaauw R, Fredericks E, Visser J, Roux S. Randomized clinical trial: effect of Lactobacillus plantarum 299 v on symptoms of irritable bowel syndrome. Nutrition 2014;30:1151-1157. https://doi.org/10.1016/j.nut.2014.02.010
- 28. Whorwell PJ, Altringer L, Morel J, Bond Y, Charbonneau D, O'Mahony L, Kiely B, Shanahan F, Quigley EM. Efficacy of an encapsulated probiotic Bifidobacterium infantis 35624 in women with irritable bowel syndrome. Am J Gastroenterol 2006;101:1581-1590. https://doi.org/10.1111/j.1572-0241.2006.00734.x
- 29. Ringel-Kulka T, McRorie J, Ringel Y. Multi-center, double-blind, randomized, placebo-controlled, parallel-group study to evaluate the benefit of the probiotic Bifidobacterium infantis 35624 in non-patients with symptoms of abdominal discomfort and bloating. Am J Gastroenterol 2017;112:145-151. https://doi.org/10.1038/ajg.2016.511
- 30. Markowiak-Kopeć P, Śliżewska K. The effect of probiotics on the production of short-chain fatty acids by human intestinal microbiome. Nutrients 2020;12:1107. https://doi.org/10.3390/nu12041107
- 31. Enck P, Zimmermann K, Menke G, Müller-Lissner S, Martens U, Klosterhalfen S. A mixture of Escherichia coli (DSM 17252) and Enterococcus faecalis (DSM 16440) for treatment of the irritable bowel syndrome: a randomized controlled trial with primary care physicians. Neurogastroenterol Motil 2008;20:1103-1109. https://doi.org/10.1111/j.1365-2982.2008.01156.x
- 32. Enck P, Zimmermann K, Menke G, Klosterhalfen S. Randomized controlled treatment trial of irritable bowel syndrome with a probiotic E.-coli preparation (DSM17252) compared to placebo. Z Gastroenterol 2009;47:209-214. https://doi.org/10.1055/s-2008-1027702
- 33. Ludidi S, Jonkers DM, Koning CJ, Kruimel JW, Mulder L, van der Vaart IB, Conchillo JM, Masclee AA. Randomized clinical trial on the effect of a multispecies probiotic on visceroperception in hypersensitive IBS patients. Neurogastroenterol Motil 2014;26:705-714. https://doi.org/10.1111/nmo.12320
- 34. Mack I, Schwille-Kiuntke J, Mazurak N, Niesler B, Zimmermann K, Mönnikes H, Enck P. A nonviable probiotic in irritable bowel syndrome: a randomized, double-blind, placebo-controlled, multicenter study. Clin Gastroenterol Hepatol 2022;20:1039-1047. https://doi.org/10.1016/j.cgh.2021.06.028
- 35. Quigley EM, Markinson L, Stevenson A, Treasure FP, Lacy BE. Randomised clinical trial: efficacy and safety of the live biotherapeutic product MRx1234 in patients with irritable bowel syndrome. Aliment Pharmacol Ther 2023;57:81-93. https://doi.org/10.1111/apt.17310
- 36. Preston K, Krumian R, Hattner J, de Montigny D, Stewart M, Gaddam S. Lactobacillus acidophilus CL1285, Lactobacillus casei LBC80R and Lactobacillus rhamnosus CLR2 improve quality-of-life and IBS symptoms: a double-blind, randomised, placebo-controlled study. Benef Microbes 2018;9:697-706. https://doi.org/10.3920/BM2017.0105
- 37. Chang YH, Choi YJ, Shin CM, Moon JS, Kim TY, Yoon H, Park YS, Kim N, Lee DH. Efficacy of quadruple-coated probiotics in patients with irritable bowel syndrome: a randomized, double-blind, placebo-controlled, parallel-group study. J Neurogastroenterol Motil 2024;30:73-86. https://doi.org/10.5056/jnm23036
- 38. Mullish BH, Michael DR, Dabcheva M, Webberley TS, Coates N, John DA, Wang D, Luo Y, Plummer SF, Marchesi JR. A double-blind, randomized, placebo-controlled study assessing the impact of probiotic supplementation on the symptoms of irritable bowel syndrome in females. Neurogastroenterol Motil 2024;36:e14751. https://doi.org/10.1111/nmo.14751
- 39. Tian Y, Zuo L, Guo Q, Li J, Hu Z, Zhao K, Li C, Li X, Zhou J, Zhou Y, Li XA. Potential role of fecal microbiota in patients with constipation. Ther Adv Gastroenterol 2020;13:1756284820968423. https://doi.org/10.1177/1756284820968423
- 40. Li YQ, Yan XY, Xiao XJ, Ma PT, Wang SQ, Liu HL, Zhang W, Chen M, Yao JP, Li Y. The gut microbiome and metabolites are altered and interrelated in patients with functional constipation. Front Microbiol 2023;14:1320567. https://doi.org/10.3389/fmicb.2023.1320567
- 41. Sekirov I, Russell SL, Antunes LC, Finlay BB. Gut microbiota in health and disease. Physiol Rev 2010;90:859-904. https://doi.org/10.1152/physrev.00045.2009
- 42. Huang LS, Kong C, Gao RY, Yan X, Yu HJ, Wen B, Zhu Q, Shen TY, Sun ZL, Qin HL. Analysis of fecal microbiota in patients with functional constipation undergoing treatment with synbiotics. Eur J Clin Microbiol Infect Dis 2018;37:555-563. https://doi.org/10.1007/s10096-017-3149-7
- 43. Chen Q, Chen D, Gao X, Jiang Y, Yu T, Jiang L, Tang Y. Association between fecal short-chain fatty acid levels and constipation severity in subjects with slow transit constipation. Eur J Gastroenterol Hepatol 2024;36:394-403. https://doi.org/10.1097/MEG.0000000000002734
- 44. Zhuang M, Shang W, Ma Q, Strappe P, Zhou Z. Abundance of probiotics and butyrate-production microbiome manages constipation via short-chain fatty acids production and hormones secretion. Mol Nutr Food Res 2019;63:e1801187. https://doi.org/10.1002/mnfr.201801187
- 45. Barberio B, Judge C, Savarino EV, Ford AC. Global prevalence of functional constipation according to the Rome criteria: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2021;6:638-648. https://doi.org/10.1016/S2468-1253(21)00111-4
- 46. Ghoshal UC, Srivastava D, Verma A, Misra A. Slow transit constipation associated with excess methane production and its improvement following rifaximin therapy: a case report. J Neurogastroenterol Motil 2011;17:185-188. https://doi.org/10.5056/jnm.2011.17.2.185
- 47. Raskov H, Burcharth J, Pommergaard HC, Rosenberg J. Irritable bowel syndrome, the microbiota and the gut-brain axis. Gut Microbes 2016;7:365-383. https://doi.org/10.1080/19490976.2016.1218585
- 48. Iancu MA, Profir M, Roşu OA, Ionescu RF, Cretoiu SM, Gaspar BS. Revisiting the intestinal microbiome and its role in diarrhea and constipation. Microorganisms 2023;11:2177. https://doi.org/10.3390/microorganisms11092177
- 49. Simrén M, Tack J. New treatments and therapeutic targets for IBS and other functional bowel disorders. Nat Rev Gastroenterol Hepatol 2018;15:589-605. https://doi.org/10.1038/s41575-018-0034-5
- 50. Del Piano M, Carmagnola S, Anderloni A, Andorno S, Ballarè M, Balzarini M, Montino F, Orsello M, Pagliarulo M, Sartori M, Tari R, Sforza F, Capurso L. The use of probiotics in healthy volunteers with evacuation disorders and hard stools: a double-blind, randomized, placebo-controlled study. J Clin Gastroenterol 2010;44 Suppl 1:S30-S34. https://doi.org/10.1097/MCG.0b013e3181ee31c3
- 51. Fateh R, Iravani S, Frootan M, Rasouli MR, Saadat S. Synbiotic preparation in men suffering from functional constipation: a randomised controlled trial. Swiss Med Wkly 2011;141:w13239. https://doi.org/10.4414/smw.2011.13239
- 52. Favretto DC, Pontin B, Moreira TR. Effect of the consumption of a cheese enriched with probiotic organisms (Bifidobacterium lactis bi-07) in improving symptoms of constipation. Arq Gastroenterol 2013;50:196-201. https://doi.org/10.1590/S0004-28032013000200035
- 53. Mazlyn MM, Nagarajah LH, Fatimah A, Norimah AK, Goh KL. Effects of a probiotic fermented milk on functional constipation: a randomized, double-blind, placebo-controlled study. J Gastroenterol Hepatol 2013;28:1141-1147. https://doi.org/10.1111/jgh.12168
- 54. Waitzberg DL, Logullo LC, Bittencourt AF, Torrinhas RS, Shiroma GM, Paulino NP, Teixeira-da-Silva ML. Effect of synbiotic in constipated adult women: a randomized, double-blind, placebo-controlled study of clinical response. Clin Nutr 2013;32:27-33. https://doi.org/10.1016/j.clnu.2012.08.010
- 55. Ojetti V, Ianiro G, Tortora A, D'Angelo G, Di Rienzo TA, Bibbò S, Migneco A, Gasbarrini A. The effect of Lactobacillus reuteri supplementation in adults with chronic functional constipation: a randomized, double-blind, placebo-controlled trial. J Gastrointestin Liver Dis 2014;23:387-391. https://doi.org/10.15403/jgld.2014.1121.234.elr
- 56. Ding C, Ge X, Zhang X, Tian H, Wang H, Gu L, Gong J, Zhu W, Li N. Efficacy of synbiotics in patients with slow transit constipation: a prospective randomized trial. Nutrients 2016;8:605. https://doi.org/10.3390/nu8100605
- 57. Cudmore S, Doolan A, Lacey S, Shanahan F. A randomised, double-blind, placebo-controlled clinical study: the effects of a synbiotic, Lepicol, in adults with chronic, functional constipation. Int J Food Sci Nutr 2017;68:366-377. https://doi.org/10.1080/09637486.2016.1244661
- 58. Ibarra A, Latreille-Barbier M, Donazzolo Y, Pelletier X, Ouwehand AC. Effects of 28-day Bifidobacterium animalis subsp. lactis HN019 supplementation on colonic transit time and gastrointestinal symptoms in adults with functional constipation: a double-blind, randomized, placebo-controlled, and dose-ranging trial. Gut Microbes 2018;9:236-251. https://doi.org/10.1080/19490976.2017.1412908
- 59. Lim YJ, Jamaluddin R, Hazizi AS, Chieng JY. Effects of synbiotics among constipated adults in Serdang, Selangor, Malaysia: a randomised, double-blind, placebo-controlled trial. Nutrients 2018;10:824. https://doi.org/10.3390/nu10070824
- 60. Dimidi E, Zdanaviciene A, Christodoulides S, Taheri S, Louis P, Duncan PI, Emami N, Crabbé R, De Castro CA, McLean P, Bergonzelli GE, Whelan K, Mark Scott S. Randomised clinical trial: Bifidobacterium lactis NCC2818 probiotic vs placebo, and impact on gut transit time, symptoms, and gut microbiology in chronic constipation. Aliment Pharmacol Ther 2019;49:251-264. https://doi.org/10.1111/apt.15073
- 61. Martoni CJ, Evans M, Chow CT, Chan LS, Leyer G. Impact of a probiotic product on bowel habits and microbial profile in participants with functional constipation: a randomized controlled trial. J Dig Dis 2019;20:435-446. https://doi.org/10.1111/1751-2980.12797
- 62. Botelho PB, Ferreira MVR, Araújo AM, Mendes MM, Nakano EY. Effect of multispecies probiotic on gut microbiota composition in individuals with intestinal constipation: a double-blind, placebo-controlled randomized trial. Nutrition 2020;78:110890. https://doi.org/10.1016/j.nut.2020.110890
- 63. Madempudi RS, Neelamraju J, Ahire JJ, Gupta SK, Shukla VK. Bacillus coagulans unique IS2 in constipation: a double-blind, placebo-controlled study. Probiotics Antimicrob Proteins 2020;12:335-342. https://doi.org/10.1007/s12602-019-09542-9
- 64. Kang S, Park MY, Brooks I, Lee J, Kim SH, Kim JY, Oh B, Kim JW, Kwon O. Spore-forming Bacillus coagulans SNZ 1969 improved intestinal motility and constipation perception mediated by microbial alterations in healthy adults with mild intermittent constipation: a randomized controlled trial. Food Res Int 2021;146:110428. https://doi.org/10.1016/j.foodres.2021.110428
- 65. Wang R, Sun J, Li G, Zhang M, Niu T, Kang X, Zhao H, Chen J, Sun E, Li Y. Effect of Bifidobacterium animalis subsp. lactis MN-Gup on constipation and the composition of gut microbiota. Benef Microbes 2021;12:31-42. https://doi.org/10.3920/BM2020.0023
- 66. Mitelmão FC, Häckel K, Bergamaschi CC, Gerenutti M, Silva MT, Balcão VM, Vila MM. The effect of probiotics on functional constipation in adults: a randomized, double-blind controlled trial. Medicine (Baltimore) 2022;101:e31185. https://doi.org/10.1097/MD.0000000000031185
- 67. Takeda T, Asaoka D, Nojiri S, Yanagisawa N, Nishizaki Y, Osada T, Koido S, Nagahara A, Katsumata N, Odamaki T, Xiao JZ, Ohkusa T, Sato N. Usefulness of Bifidobacterium longum BB536 in elderly individuals with chronic constipation: a randomized controlled trial. Am J Gastroenterol 2023;118:561-568. https://doi.org/10.14309/ajg.0000000000002028
- 68. Wang L, Wang L, Tian P, Wang B, Cui S, Zhao J, Zhang H, Qian L, Wang Q, Chen W, Wang G. A randomised, double-blind, placebo-controlled trial of Bifidobacterium bifidum CCFM16 for manipulation of the gut microbiota and relief from chronic constipation. Food Funct 2022;13:1628-1640. https://doi.org/10.1039/d1fo03896f
- 69. Lai H, Li Y, He Y, Chen F, Mi B, Li J, Xie J, Ma G, Yang J, Xu K, Liao X, Yin Y, Liang J, Kong L, Wang X, Li Z, Shen Y, Dang S, Zhang L, Wu Q, Zeng L, Shi L, Zhang X, Tian T, Liu X. Effects of dietary fibers or probiotics on functional constipation symptoms and roles of gut microbiota: a double-blinded randomized placebo trial. Gut Microbes 2023;15:2197837. https://doi.org/10.1080/19490976.2023.2197837
- 70. Ma T, Yang N, Xie Y, Li Y, Xiao Q, Li Q, Jin H, Zheng L, Sun Z, Zuo K, Kwok LY, Zhang H, Lu N, Liu W. Effect of the probiotic strain, Lactiplantibacillus plantarum P9, on chronic constipation: a randomized, double-blind, placebo-controlled study. Pharmacol Res 2023;191:106755. https://doi.org/10.1016/j.phrs.2023.106755
- 71. Cheng J, Gao C, Ala-Jaakkola R, Forssten SD, Saarinen M, Hibberd A, Ouwehand AC, Ibarra A, Li D, Nordlund A, Wang Y, Shen X, Peng H, Wan X, Meng X. Eight-week supplementation with Bifidobacterium lactis HN019 and functional constipation: a randomized clinical trial. JAMA Netw Open 2024;7:e2436888. https://doi.org/10.1001/jamanetworkopen.2024.36888
- 72. Salo E, Roche D, Gomez-Martinez VB, Cruz-Domenech JM, Garcia-Mora LG, Gabernet-Castello C, Freixenet N. Bifidobacterium animalis subsp. lactis BLa80 regulates the intestinal habit in adults with chronic constipation: a multicentre, randomised, double-blind, placebo-controlled study. Benef Microbes 2024;15:679-688. https://doi.org/10.1163/18762891-bja00038
- 73. Jin YJ, Park YJ, Choi J, Kim MS, Min U, Lim J, Kang J, Lee DY, Kim BY. Impact of probiotic formula (Lacto-5X) on constipation: improvements in gastrointestinal symptoms, gut microbiome, and metabolites. J Microbiol Biotechnol 2025;35:e2412056. https://doi.org/10.4014/jmb.2412.12056
- 74. Roos S, Dahlgren AL, Mao YK, Pallin A, Stanisz AM, Forsythe P, Kunze W, Hellström PM. Therapeutic value of Lactobacillus gasseri 345A in chronic constipation. Neurogastroenterol Motil 2025;37:e70012. https://doi.org/10.1111/nmo.70012
- 75. Deng X, Liang C, Zhou L, Shang X, Hui X, Hou L, Wang Y, Liu W, Liang S, Yao L, Yang K, Li X. Network meta-analysis of probiotics, prebiotics, and synbiotics for the treatment of chronic constipation in adults. Eur J Nutr 2024;63:1999-2010. https://doi.org/10.1007/s00394-024-03410-1
- 76. Xia J, Liu T, Wan R, Zhang J, Fu Q. Global burden and trends of the Clostridioides difficile infection-associated diseases from 1990 to 2021: an observational trend study. Ann Med 2025;57:2451762. https://doi.org/10.1080/07853890.2025.2451762
- 77. Safdar N, Barigala R, Said A, McKinley L. Feasibility and tolerability of probiotics for prevention of antibiotic-associated diarrhoea in hospitalized US military veterans. J Clin Pharm Ther 2008;33:663-668. https://doi.org/10.1111/j.1365-2710.2008.00980.x
- 78. Rajkumar C, Wilks M, Islam J, Ali K, Raftery J, Davies KA, Timeyin J, Cheek E, Cohen J. Do probiotics prevent antibiotic-associated diarrhoea?: results of a multicentre randomized placebo-controlled trial. J Hosp Infect 2020;105:280-288. https://doi.org/10.1016/j.jhin.2020.01.018
- 79. Allen SJ, Wareham K, Wang D, Bradley C, Hutchings H, Harris W, Dhar A, Brown H, Foden A, Gravenor MB, Mack D. Lactobacilli and bifidobacteria in the prevention of antibiotic-associated diarrhoea and Clostridium difficile diarrhoea in older inpatients (PLACIDE): a randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2013;382:1249-1257. https://doi.org/10.1016/S0140-6736(13)61218-0
- 80. Zhang DM, Xu BB, Yu L, Zheng LF, Chen LP, Wang W. A prospective control study of Saccharomyces boulardii in prevention of antibiotic-associated diarrhea in the older inpatients. Zhonghua Nei Ke Za Zhi 2017;56:398-401. https://doi.org/10.3760/cma.j.issn.0578-1426.2017.06.003
- 81. Pozzoni P, Riva A, Bellatorre AG, Amigoni M, Redaelli E, Ronchetti A, Stefani M, Tironi R, Molteni EE, Conte D, Casazza G, Colli A. Saccharomyces boulardii for the prevention of antibiotic-associated diarrhea in adult hospitalized patients: a single-center, randomized, double-blind, placebo-controlled trial. Am J Gastroenterol 2012;107:922-931. https://doi.org/10.1038/ajg.2012.56
- 82. Can M, Beşirbellioglu BA, Avci IY, Beker CM, Pahsa A. Prophylactic Saccharomyces boulardii in the prevention of antibiotic-associated diarrhea: a prospective study. Med Sci Monit 2006;12:PI19-PI22.
- 83. Hickson M, D’Souza AL, Muthu N, Rogers TR, Want S, Rajkumar C, Bulpitt CJ. Use of probiotic Lactobacillus preparation to prevent diarrhoea associated with antibiotics: randomised double blind placebo controlled trial. BMJ 2007;335:80. https://doi.org/10.1136/bmj.39231.599815.55
- 84. Louie T, Golan Y, Khanna S, Bobilev D, Erpelding N, Fratazzi C, Carini M, Menon R, Ruisi M, Norman JM, Faith JJ, Olle B, Li M, Silber JL, Pardi DS. VE303, a defined bacterial consortium, for prevention of recurrent Clostridioides difficile infection: a randomized clinical trial. JAMA 2023;329:1356-1366. https://doi.org/10.1001/jama.2023.4314
- 85. Chitapanarux T, Wiracha U, Winichakoon P, Salee P, Traisathit P. Efficacy and safety of Saccharomyces boulardii as adjunct therapy with Vancomycin in treating Clostridioides difficile infection: a randomized controlled trial. Sci Rep 2025;15:19326. https://doi.org/10.1038/s41598-025-04986-2
- 86. Barker AK, Duster M, Valentine S, Hess T, Archbald-Pannone L, Guerrant R, Safdar N. A randomized controlled trial of probiotics for Clostridium difficile infection in adults (PICO). J Antimicrob Chemother 2017;72:3177-3180. https://doi.org/10.1093/jac/dkx254
- 87. Plummer S, Weaver MA, Harris JC, Dee P, Hunter J. Clostridium difficile pilot study: effects of probiotic supplementation on the incidence of C. difficile diarrhoea. Int Microbiol 2004;7:59-62.
- 88. McFarland LV, Surawicz CM, Greenberg RN, Fekety R, Elmer GW, Moyer KA, Melcher SA, Bowen KE, Cox JL, Noorani Z. A randomized placebo-controlled trial of Saccharomyces boulardii in combination with standard antibiotics for Clostridium difficile disease. JAMA 1994;271:1913-1918. https://doi.org/10.1001/jama.1994.03510480037031
- 89. Wullt M, Hagslätt ML, Odenholt I. Lactobacillus plantarum 299v for the treatment of recurrent Clostridium difficile-associated diarrhoea: a double-blind, placebo-controlled trial. Scand J Infect Dis 2003;35:365-367. https://doi.org/10.1080/00365540310010985
- 90. Allegretti JR, Kelly CR, Louie T, Fischer M, Hota S, Misra B, Van Hise NW, Yen E, Bullock JS, Silverman M, Davis I, McGill SK, Pardi DS, Orenstein R, Grinspan A, El-Nachef N, Feuerstadt P, Borody TJ, Khanna S, Budree S, Kassam Z. Safety and tolerability of CP101, a full-spectrum, oral microbiome therapeutic for the prevention of recurrent Clostridioides difficile infection: a phase 2 randomized controlled trial. Gastroenterology 2025;168:357-366. https://doi.org/10.1053/j.gastro.2024.09.030
- 91. Shah PJ, Halawi H, Kay J, Akogun A, Wise S, Aly S, Daoura N, Putney D. A single-center, retrospective cohort study evaluating the use of probiotics for the prevention of hospital-onset Clostridioides difficile infection in hospitalized patients receiving intravenous antibiotics. Hosp Pharm 2023;58:57-61. https://doi.org/10.1177/00185787221120153
- 92. Heil EL, Harris AD, Brown C, Seung H, Thom KA, von Rosenvinge E, Sorongon S, Pineles L, Goodman KE, Leekha S. A multicenter evaluation of probiotic use for the primary prevention of Clostridioides difficile infection. Clin Infect Dis 2021;73:1330-1337. https://doi.org/10.1093/cid/ciab417
- 93. Goldenberg JZ, Yap C, Lytvyn L, Lo CK, Beardsley J, Mertz D, Johnston BC. Probiotics for the prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database Syst Rev 2017;12:CD006095. https://doi.org/10.1002/14651858.CD006095.pub4
- 94. Shen NT, Maw A, Tmanova LL, Pino A, Ancy K, Crawford CV, Simon MS, Evans AT. Timely use of probiotics in hospitalized adults prevents Clostridium difficile infection: a systematic review with meta-regression analysis. Gastroenterology 2017;152:1889-1900. https://doi.org/10.1053/j.gastro.2017.02.003
- 95. Kelly CR, Fischer M, Allegretti JR, LaPlante K, Stewart DB, Limketkai BN, Stollman NH. ACG Clinical Guidelines: prevention, diagnosis, and treatment of Clostridioides difficile infections. Am J Gastroenterol 2021;116:1124-1147. https://doi.org/10.14309/ajg.0000000000001278
- 96. Johnson S, Lavergne V, Skinner AM, Gonzales-Luna AJ, Garey KW, Kelly CP, Wilcox MH. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of Clostridioides difficile infection in adults. Clin Infect Dis 2021;73:755-757. https://doi.org/10.1093/cid/ciab718
- 97. van Prehn J, Reigadas E, Vogelzang EH, Bouza E, Hristea A, Guery B, Krutova M, Norén T, Allerberger F, Coia JE, Goorhuis A, van Rossen TM, Ooijevaar RE, Burns K, Scharvik Olesen BR, Tschudin-Sutter S, Wilcox MH, Vehreschild MJ, Fitzpatrick F, Kuijper EJ. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin Microbiol Infect 2021;27 Suppl 2:S1-S21. https://doi.org/10.1016/j.cmi.2021.09.038
- 98. Eeuwijk J, Ferreira G, Yarzabal JP, Robert-Du Ry van Beest Holle M. A systematic literature review on risk factors for and timing of Clostridioides difficile infection in the United States. Infect Dis Ther 2024;13:273-298. https://doi.org/10.1007/s40121-024-00919-0
- 99. Young EH, Strey KA, Lee GC, Carlson TJ, Koeller JM, Reveles KR. Clostridioides difficile infection treatment and outcome disparities in a national sample of United States hospitals. Antibiotics (Basel) 2022;11:1203. https://doi.org/10.3390/antibiotics11091203
- 100. Vemuri R, Sylvia KE, Klein SL, Forster SC, Plebanski M, Eri R, Flanagan KL. The microgenderome revealed: sex differences in bidirectional interactions between the microbiota, hormones, immunity and disease susceptibility. Semin Immunopathol 2019;41:265-275. https://doi.org/10.1007/s00281-018-0716-7
- 101. Di Bella S, Sanson G, Monticelli J, Zerbato V, Principe L, Giuffrè M, Pipitone G, Luzzati R. Clostridioides difficile infection: history, epidemiology, risk factors, prevention, clinical manifestations, treatment, and future options. Clin Microbiol Rev 2024;37:e0013523. https://doi.org/10.1128/cmr.00135-23
- 102. Ter Horst R, Jaeger M, Smeekens SP, Oosting M, Swertz MA, Li Y, Kumar V, Diavatopoulos DA, Jansen AF, Lemmers H, Toenhake-Dijkstra H, van Herwaarden AE, Janssen M, van der Molen RG, Joosten I, Sweep FC, Smit JW, Netea-Maier RT, Koenders MM, Xavier RJ, van der Meer JW, Dinarello CA, Pavelka N, Wijmenga C, Notebaart RA, Joosten LA, Netea MG. Host and environmental factors influencing individual human cytokine responses. Cell 2016;167:1111-1124. https://doi.org/10.1016/j.cell.2016.10.018
- 103. Yoon K, Kim N. Roles of sex hormones and gender in the gut microbiota. J Neurogastroenterol Motil 2021;27:314-325. https://doi.org/10.5056/jnm20208
- 104. Kim N. Sex difference of gut microbiota. In: Kim N, editor. Sex/gender-specific medicine in the gastrointestinal diseases. Springer Singapore; 2022. p. 363-377. https://doi.org/10.1007/978-981-19-0120-1_22
- 105. Gomez A, Luckey D, Taneja V. The gut microbiome in autoimmunity: sex matters. Clin Immunol 2015;159:154-162. https://doi.org/10.1016/j.clim.2015.04.016
- 106. Kim YS, Kim N. Sex-gender differences in irritable bowel syndrome. J Neurogastroenterol Motil 2018;24:544-558. https://doi.org/10.5056/jnm18082
- 107. Ait-Belgnaoui A, Eutamene H, Houdeau E, Bueno L, Fioramonti J, Theodorou V. Lactobacillus farciminis treatment attenuates stress-induced overexpression of Fos protein in spinal and supraspinal sites after colorectal distension in rats. Neurogastroenterol Motil 2009;21:567-573. https://doi.org/10.1111/j.1365-2982.2009.01280.x
- 108. Distrutti E, Monaldi L, Ricci P, Fiorucci S. Gut microbiota role in irritable bowel syndrome: new therapeutic strategies. World J Gastroenterol 2016;22:2219-2241. https://doi.org/10.3748/wjg.v22.i7.2219
- 109. Tremaroli V, Bäckhed F. Functional interactions between the gut microbiota and host metabolism. Nature 2012;489:242-249. https://doi.org/10.1038/nature11552
- 110. Rivière A, Selak M, Lantin D, Leroy F, De Vuyst L. Bifidobacteria and butyrate-producing colon bacteria: importance and strategies for their stimulation in the human gut. Front Microbiol 2016;7:979. https://doi.org/10.3389/fmicb.2016.00979
- 111. Yoon K, Kim N. The effect of microbiota on colon carcinogenesis. J Cancer Prev 2018;23:117-125. https://doi.org/10.15430/JCP.2018.23.3.117
- 112. Louis P, Hold GL, Flint HJ. The gut microbiota, bacterial metabolites and colorectal cancer. Nat Rev Microbiol 2014;12:661-672. https://doi.org/10.1038/nrmicro3344
- 113. Shastri P, McCarville J, Kalmokoff M, Brooks SP, Green-Johnson JM. Sex differences in gut fermentation and immune parameters in rats fed an oligofructose-supplemented diet. Biol Sex Differ 2015;6:13. https://doi.org/10.1186/s13293-015-0031-0
- 114. Ou J, Carbonero F, Zoetendal EG, DeLany JP, Wang M, Newton K, Gaskins HR, O'Keefe SJ. Diet, microbiota, and microbial metabolites in colon cancer risk in rural Africans and African Americans. Am J Clin Nutr 2013;98:111-120. https://doi.org/10.3945/ajcn.112.056689
- 115. Mueller S, Saunier K, Hanisch C, Norin E, Alm L, Midtvedt T, Cresci A, Silvi S, Orpianesi C, Verdenelli MC, Clavel T, Koebnick C, Zunft HJ, Doré J, Blaut M. Differences in fecal microbiota in different European study populations in relation to age, gender, and country: a cross-sectional study. Appl Environ Microbiol 2006;72:1027-1033. https://doi.org/10.1128/AEM.72.2.1027-1033.2006
- 116. Mu Q, Zhang H, Liao X, Lin K, Liu H, Edwards MR, Ahmed SA, Yuan R, Li L, Cecere TE, Branson DB, Kirby JL, Goswami P, Leeth CM, Read KA, Oestreich KJ, Vieson MD, Reilly CM, Luo XM. Control of lupus nephritis by changes of gut microbiota. Microbiome 2017;5:73. https://doi.org/10.1186/s40168-017-0300-8
- 117. Mazurak N, Broelz E, Storr M, Enck P. Probiotic therapy of the irritable bowel syndrome: why is the evidence still poor and what can be done about it? J Neurogastroenterol Motil 2015;21:471-485. https://doi.org/10.5056/jnm15071
- 118. Lee JY, Kim N, Nam RH, Sohn SH, Lee SM, Choi D, Yoon H, Kim YS, Lee HS, Lee DH. Probiotics reduce repeated water avoidance stress-induced colonic microinflammation in Wistar rats in a sex-specific manner. PLoS One 2017;12:e0188992. https://doi.org/10.1371/journal.pone.0188992
- 119. Choi SI, Kim N, Nam RH, Jang JY, Kim EH, Ha S, Kang K, Lee W, Shin CM, Lee DH. Sex difference in the effect of bifidobacterium longum on repeated water avoidance stress-induced gut dysbiosis in Wistar rats. J Cancer Prev 2024;29:16-23. https://doi.org/10.15430/JCP.23.042
- 120. Choi SI, Kim N, Nam RH, Jang JY, Kim EH, Ha S, Kang K, Lee W, Choi H, Kim YR, Seok YJ, Shin CM, Lee DH. The protective effect of Roseburia faecis against repeated water avoidance stress-induced irritable bowel syndrome in a Wister rat model. J Cancer Prev 2023;28:93-105. https://doi.org/10.15430/JCP.2023.28.3.93
- 121. Choi Y, Choi SI, Kim N, Nam RH, Jang JY, Na HY, Shin CM, Lee DH, Min H, Kim YR, Seok YJ. Effect of Clostridium butyricum on high-fat diet-induced intestinal inflammation and production of short-chain fatty acids. Dig Dis Sci 2023;68:2427-2440. https://doi.org/10.1007/s10620-023-07835-2
- 122. Choi SI, Kim N, Choi Y, Nam RH, Jang JY, Cho SY. The effect of Clostridium butyricum on gut microbial changes and functional profiles of metabolism in high-fat diet-fed rats depending on age and sex. J Neurogastroenterol Motil 2024;30:236-250. https://doi.org/10.5056/jnm23096
- 123. He J, Wang W, Wu Z, Pan D, Guo Y, Cai Z, Lian L. Effect of Lactobacillus reuteri on intestinal microbiota and immune parameters: involvement of sex differences. J Funct Foods 2019;53:36-43. https://doi.org/10.1016/j.jff.2018.12.010
- 124. Singh S, Abu Y, Antoine D, Gomez D, Tao J, Truitt B, Roy S. Probiotic supplementation mitigates sex-dependent nociceptive changes and gut dysbiosis induced by prenatal opioid exposure. Gut Microbes 2025;17:2464942. https://doi.org/10.1080/19490976.2025.2464942
- 125. McFarland LV. Meta-analysis of probiotics for the prevention of antibiotic associated diarrhea and the treatment of Clostridium difficile disease. Am J Gastroenterol 2006;101:812-822. https://doi.org/10.1111/j.1572-0241.2006.00465.x
- 126. Gibson GR, Hutkins R, Sanders ME, Prescott SL, Reimer RA, Salminen SJ, Scott K, Stanton C, Swanson KS, Cani PD, Verbeke K, Reid G. Expert consensus document: the International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat Rev Gastroenterol Hepatol 2017;14:491-502. https://doi.org/10.1038/nrgastro.2017.75
- 127. Hungin AP, Mulligan C, Pot B, Whorwell P, Agréus L, Fracasso P, Lionis C, Mendive J, Philippart de Foy JM, Rubin G, Winchester C, de Wit N. Systematic review: probiotics in the management of lower gastrointestinal symptoms in clinical practice: an evidence-based international guide. Aliment Pharmacol Ther 2013;38:864-886. https://doi.org/10.1111/apt.12460
- 128. Ministry of Food and Drug Safety. Health Functional Food Code (Notice No. 2021-65). Ministry of Food and Drug Safety; 2021.
- 129. Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, Morelli L, Canani RB, Flint HJ, Salminen S, Calder PC, Sanders ME. Expert consensus document: the International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol 2014;11:506-514. https://doi.org/10.1038/nrgastro.2014.66
- 130. McFarland LV, Evans CT, Goldstein EJ. Strain-specificity and disease-specificity of probiotic efficacy: a systematic review and meta-analysis. Front Med (Lausanne) 2018;5:124. https://doi.org/10.3389/fmed.2018.00124
- 131. Fenster K, Freeburg B, Hollard C, Wong C, Rønhave Laursen R, Ouwehand AC. The production and delivery of probiotics: a review of a practical approach. Microorganisms 2019;7:83. https://doi.org/10.3390/microorganisms7030083
- 132. Santivarangkna C, Kulozik U, Foerst P. Alternative drying processes for the industrial preservation of lactic acid starter cultures. Biotechnol Prog 2007;23:302-315. https://doi.org/10.1021/bp060268f
- 133. Baral KC, Bajracharya R, Lee SH, Han HK. Advancements in the pharmaceutical applications of probiotics: dosage forms and formulation technology. Int J Nanomedicine 2021;16:7535-7556. https://doi.org/10.2147/IJN.S337427
- 134. Tompkins TA, Mainville I, Arcand Y. The impact of meals on a probiotic during transit through a model of the human upper gastrointestinal tract. Benef Microbes 2011;2:295-303. https://doi.org/10.3920/BM2011.0022
- 135. Thaiss CA, Levy M, Korem T, Dohnalová L, Shapiro H, Jaitin DA, David E, Winter DR, Gury-BenAri M, Tatirovsky E, Tuganbaev T, Federici S, Zmora N, Zeevi D, Dori-Bachash M, Pevsner-Fischer M, Kartvelishvily E, Brandis A, Harmelin A, Shibolet O, Halpern Z, Honda K, Amit I, Segal E, Elinav E. Microbiota diurnal rhythmicity programs host transcriptome oscillations. Cell 2016;167:1495-1510. https://doi.org/10.1016/j.cell.2016.11.003
- 136. Didari T, Mozaffari S, Nikfar S, Abdollahi M. Effectiveness of probiotics in irritable bowel syndrome: updated systematic review with meta-analysis. World J Gastroenterol 2015;21:3072-3084. https://doi.org/10.3748/wjg.v21.i10.3072
- 137. Zmora N, Zilberman-Schapira G, Suez J, Mor U, Dori-Bachash M, Bashiardes S, Kotler E, Zur M, Regev-Lehavi D, Brik RB, Federici S, Cohen Y, Linevsky R, Rothschild D, Moor AE, Ben-Moshe S, Harmelin A, Itzkovitz S, Maharshak N, Shibolet O, Shapiro H, Pevsner-Fischer M, Sharon I, Halpern Z, Segal E, Elinav E. Personalized gut mucosal colonization resistance to empiric probiotics is associated with unique host and microbiome features. Cell 2018;174:1388-1405. https://doi.org/10.1016/j.cell.2018.08.041
- 138. Blekhman R, Goodrich JK, Huang K, Sun Q, Bukowski R, Bell JT, Spector TD, Keinan A, Ley RE, Gevers D, Clark AG. Host genetic variation impacts microbiome composition across human body sites. Genome Biol 2015;16:191. https://doi.org/10.1186/s13059-015-0759-1
- 139. Underwood MA. Probiotics and the prevention of necrotizing enterocolitis. J Pediatr Surg 2019;54:405-412. https://doi.org/10.1016/j.jpedsurg.2018.08.055
- 140. Hutchinson AN, Bergh C, Kruger K, Sűsserová M, Allen J, Améen S, Tingö L. The effect of probiotics on health outcomes in the elderly: a systematic review of randomized, placebo-controlled studies. Microorganisms 2021;9:1344. https://doi.org/10.3390/microorganisms9061344
- 141. Kovatcheva-Datchary P, Nilsson A, Akrami R, Lee YS, De Vadder F, Arora T, Hallen A, Martens E, Björck I, Bäckhed F. Dietary fiber-induced improvement in glucose metabolism is associated with increased abundance of prevotella. Cell Metab 2015;22:971-982. https://doi.org/10.1016/j.cmet.2015.10.001
- 142. Derwa Y, Gracie DJ, Hamlin PJ, Ford AC. Systematic review with meta-analysis: the efficacy of probiotics in inflammatory bowel disease. Aliment Pharmacol Ther 2017;46:389-400. https://doi.org/10.1111/apt.14203
- 143. Imhann F, Bonder MJ, Vich Vila A, Fu J, Mujagic Z, Vork L, Tigchelaar EF, Jankipersadsing SA, Cenit MC, Harmsen HJ, Dijkstra G, Franke L, Xavier RJ, Jonkers D, Wijmenga C, Weersma RK, Zhernakova A. Proton pump inhibitors affect the gut microbiome. Gut 2016;65:740-748. https://doi.org/10.1136/gutjnl-2015-310376
- 144. Hempel S, Newberry S, Ruelaz A, Wang Z, Miles JN, Suttorp MJ, Johnsen B, Shanman R, Slusser W, Fu N, Smith A, Roth B, Polak J, Motala A, Perry T, Shekelle PG. Safety of probiotics used to reduce risk and prevent or treat disease. Evid Rep Technol Assess (Full Rep) 2011;(200):1-645.
- 145. Doron S, Snydman DR. Risk and safety of probiotics. Clin Infect Dis 2015;60 Suppl 2:S129-S134. https://doi.org/10.1093/cid/civ085
- 146. Merenstein D, Pot B, Leyer G, Ouwehand AC, Preidis GA, Elkins CA, Hill C, Lewis ZT, Shane AL, Zmora N, Petrova MI, Collado MC, Morelli L, Montoya GA, Szajewska H, Tancredi DJ, Sanders ME. Emerging issues in probiotic safety: 2023 perspectives. Gut Microbes 2023;15:2185034. https://doi.org/10.1080/19490976.2023.2185034
- 147. Wang Y, Tan W, Li X, Yang G, Wang Y, Liao J, Lu A, Zhang G, Chen K, Yang L, Li W. A pharmacovigilance study on probiotic preparations based on the FDA Adverse Event Reporting System from 2005 to 2023. Front Cell Infect Microbiol 2025;15:1455735. https://doi.org/10.3389/fcimb.2025.1455735
- 148. Besselink MG, van Santvoort HC, Buskens E, Boermeester MA, van Goor H, Timmerman HM, Nieuwenhuijs VB, Bollen TL, van Ramshorst B, Witteman BJ, Rosman C, Ploeg RJ, Brink MA, Schaapherder AF, Dejong CH, Wahab PJ, van Laarhoven CJ, van der Harst E, van Eijck CH, Cuesta MA, Akkermans LM, Gooszen HG. Probiotic prophylaxis in predicted severe acute pancreatitis: a randomised, double-blind, placebo-controlled trial. Lancet 2008;371:651-659. https://doi.org/10.1016/S0140-6736(08)60207-X
- 149. U.S. Food and Drug Administration. Risk of invasive disease in preterm infants given probiotics formulated to contain live bacteria or yeast. U.S. Food and Drug Administration; 2023.
- 150. Rannikko J, Holmberg V, Karppelin M, Arvola P, Huttunen R, Mattila E, Kerttula N, Puhto T, Tamm Ü, Koivula I, Vuento R, Syrjänen J, Hohenthal U. Fungemia and other fungal infections associated with use of Saccharomyces boulardii probiotic supplements. Emerg Infect Dis 2021;27:2090-2096. https://doi.org/10.3201/eid2708.210018
- 151. Pace F, Macchini F, Massimo Castagna V. Safety of probiotics in humans: a dark side revealed? Dig Liver Dis 2020;52:981-985. https://doi.org/10.1016/j.dld.2020.04.029
- 152. Kullar R, Goldstein EJ, Johnson S, McFarland LV. Lactobacillus bacteremia and probiotics: a review. Microorganisms 2023;11:896. https://doi.org/10.3390/microorganisms11040896
- 153. Bongaerts GP, Severijnen RS. A reassessment of the PROPATRIA study and its implications for probiotic therapy. Nat Biotechnol 2016;34:55-63. https://doi.org/10.1038/nbt.3436

 , Seon-Young Park3
, Seon-Young Park3