A 30-year-old woman presented with a progressive, stabbing left-sided hemicranial headache, dysphagia, bilateral hearing loss, and facial paralysis. Her recent medical history was notable for left-sided otomastoiditis, for which she had undergone tympanomastoidectomy and facial nerve decompression. Neurological examination revealed left-sided lower motor neuron facial paralysis, anisocoria, and mild dysarthria. Electroneuromyography demonstrated bilateral facial nerve axonal injury, along with severe axonal injury of the left accessory nerve.
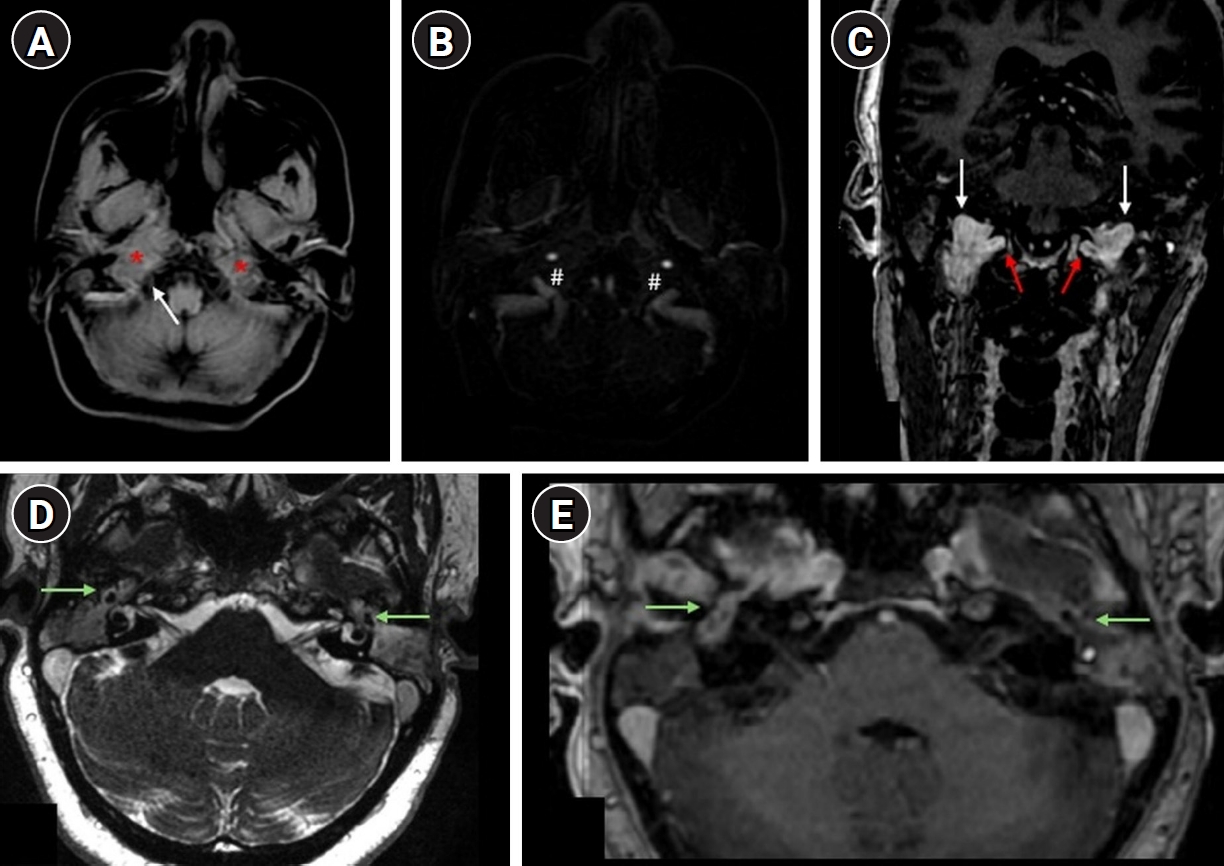
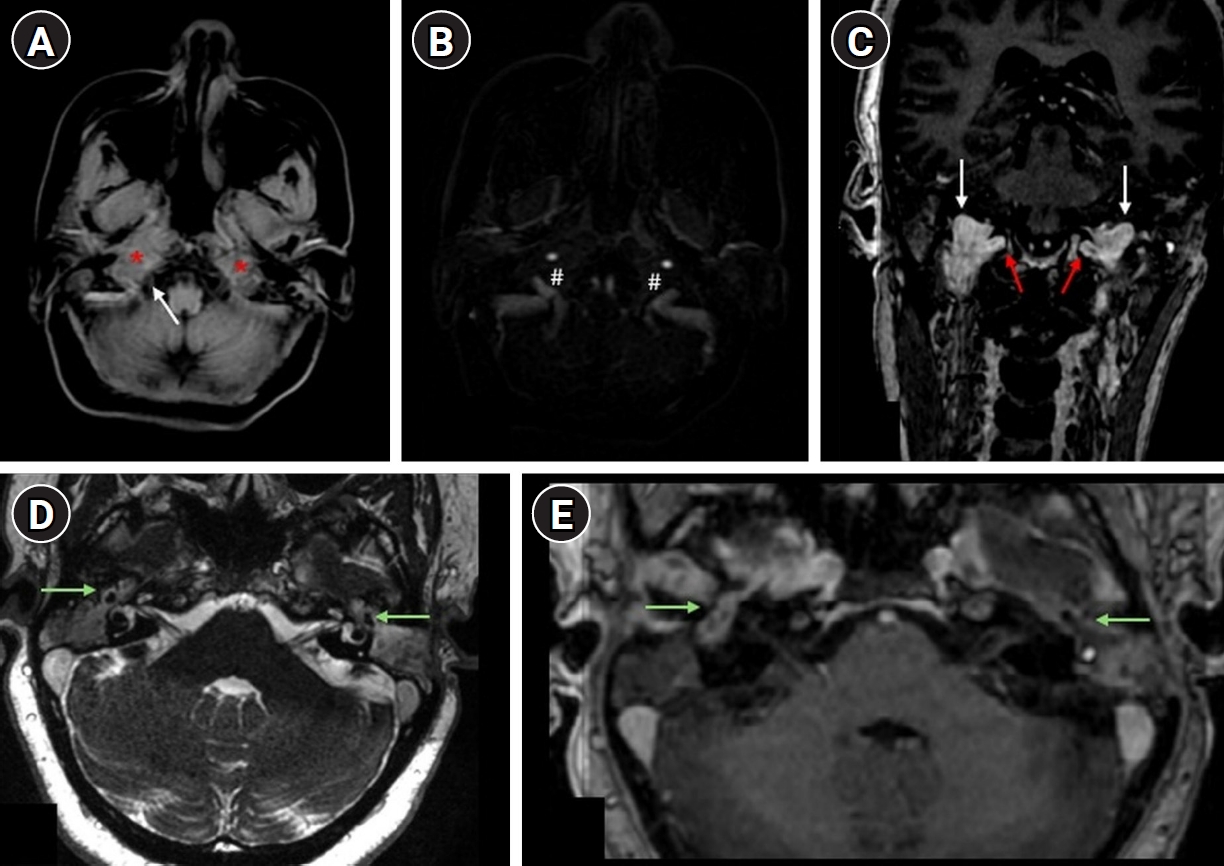
Brain magnetic resonance imaging (MRI) demonstrated homogeneous, enhancing soft-tissue thickening at the skull base, extending into the nasopharynx and involving the courses of cranial nerves IX–XII, with more prominent involvement on the right side (
Fig. 1). Additional MRI findings included enhancing soft tissue within the tympanic cavities, involving the tympanic segments of the facial nerves bilaterally. These findings provide an anatomical explanation for the facial paralysis, even in the absence of intracanalicular nerve enhancement. Although the skull base lesion was more pronounced on the right, bilateral involvement of the tympanic segments accounts for the clinical presentation. Serologic testing, including cytoplasmic antineutrophil cytoplasmic antibody (ANCA), perinuclear ANCA, anti-proteinase 3, and anti-myeloperoxidase antibodies, was negative. Histopathology reportedly demonstrated granulomatous inflammation with multinucleated giant cells. As histologic slides were not available for review in this teleradiology case, the diagnosis of granulomatosis with polyangiitis (GPA) was established based on clinicoradiologic correlation and a compatible biopsy report. Treatment with corticosteroids and rituximab was initiated. According to follow-up information from the treating team, the patient demonstrated marked clinical improvement, particularly in headache, dysphagia, and facial nerve function.
GPA is a necrotizing vasculitis that only rarely involves the central nervous system; however, cranial neuropathies related to skull base or otologic involvement may occur in fewer than 10% of patients [
1]. ANCA-negative disease is more commonly observed in cases with localized head and neck involvement and may present a diagnostic challenge. In such cases, diagnosis typically relies on tissue biopsy in conjunction with clinical and radiologic correlation, rather than serologic findings alone. Otologic manifestations are relatively common, but the association with peripheral facial paralysis remains uncommon, reported in only 8%–10% of cases [
2,
3]. The relatively young age of this patient further underscores the diagnostic complexity.
The differential diagnosis of inflammatory skull base lesions includes skull base osteomyelitis, tuberculosis, sarcoidosis, immunoglobulin G4 (IgG4)-related disease, inflammatory pseudotumor, and lymphoma. Skull base osteomyelitis was initially considered given the history of otomastoiditis; however, the presence of extensive infiltrative soft tissue, skull base foraminal involvement, and multiple cranial neuropathies was more suggestive of an inflammatory granulomatous process. Tuberculosis and sarcoidosis were not supported by the biopsy findings. IgG4-related disease and inflammatory pseudotumor were considered less likely based on the pattern of cranial nerve involvement and the clinical course. Lymphoma was also included in the differential diagnosis but was not supported by histopathologic findings. Ultimately, the diagnosis was established based on clinicoradiologic correlation and compatible biopsy findings. A limitation of this report is the unavailability of histopathologic slides for review, as this was a teleradiology case; however, the diagnosis was supported by the pathology report, clinical presentation, imaging findings, exclusion of alternative diagnoses, and response to treatment.
This case highlights the importance of considering GPA in the differential diagnosis of skull base lesions that may mimic neoplastic or infectious processes. Early diagnosis and prompt initiation of immunosuppressive therapy are essential to prevent irreversible neurological sequelae [
4].
Informed consent was obtained from the patient for publication of this case and the accompanying images.
-
Authors’ contribution
Conceptualization: JMAM, GA, MLD. Data curation: JMAM, MLD. Methodology/formal analysis/validation: JMAM, GA, MQPS, MLD. Project administration: JMAM, GA, MLD. Funding acquisition: none. Writing–original draft: JMAM, MQPS, RAA, MLD. Writing–review & editing: JMAM, GA, RAA, MLD.
-
Conflict of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Fig. 1.Magnetic resonance imaging. (A) Axial post-contrast T1-weighted images with fat suppression; (B) axial magnetic resonance venography; (C) coronal post-contrast T1-weighted images; (D) axial FIESTA sequence; (E) axial post-contrast T1-weighted image. Amorphous enhancing soft-tissue formations are observed following intravenous contrast administration, centered in the superior portion of the carotid spaces and the prevertebral component of the paravertebral spaces (*), with extension into the jugular foramina (white arrow) and hypoglossal canals (red arrows). A mass effect with obliteration of the jugular bulbs (#) is also noted. Heterogeneously enhancing tissue is present within the tympanic cavities and adjacent mastoid air cells, infiltrating the tympanic segments of the facial nerves (green arrows). Panel (E) highlights enhancing soft tissue within the tympanic cavity involving the tympanic segment of the facial nerve.
References
- 1. Koenen L, Elbelt U, Olze H, Zappe S, Dommerich S. Granulomatosis with polyangiitis in a patient with polydipsia, facial nerve paralysis, and severe otologic complaints: a case report and review of the literature. J Med Case Rep 2022;16:291. https://doi.org/10.1186/s13256-022-03492-7
- 2. Marszał J, Bartochowska A, Yu R, Wierzbicka M. Facial nerve paresis in the course of masked mastoiditis as a revelator of GPA. Eur Arch Otorhinolaryngol 2022;279:4271-4278. https://doi.org/10.1007/s00405-021-07166-w
- 3. Odom JQ, Mangan AR, Gibson AC, Larson M, Dornhoffer JL, Saadi RA. Diagnosis and management of facial nerve palsy secondary to granulomatosis with polyangiitis: a systematic review. Am J Otolaryngol 2024;45:104132. https://doi.org/10.1016/j.amjoto.2023.104132
- 4. Kiessling PT, Marinelli JP, Peters PA, DeLone DR, Lane JI, Koster MJ, Carlson ML. Cranial base manifestations of granulomatosis with polyangiitis. Otolaryngol Head Neck Surg 2020;162:666-673. https://doi.org/10.1177/0194599820912025
Citations
Citations to this article as recorded by


 , Gustavo Andreis2
, Gustavo Andreis2